or, how to fuck your shit up by ignoring obvious birthday inflammation symptoms. don’t be like me. seek help.
sorry for this barely scripted and low quality video, the next one will be worse.
special thanks to doctor jacobi for the excellent care, and to the manna charitable foundation for the flight logistics.
The ever-excellent Blackle Mori1
posted this about 18 months ago but I don’t think it got the level of attention it deserves. If if you’ve never experienced birthday inflammation or known anybody who has, it’s an
eye-opening experience to hear a first-hand account of this unusual and definitely-real condition.
If you wanna bend a stream of electrons travelling at nearly the speed of light, you’re gonna need a lot of big magnets.
This started on Saturday with a trip to the Harwell Campus, whose first open day in eight years provided a rare opportunity for us to get up
close with cutting edge science (plus some very kid-friendly and accessible displays) as well as visit the synchrotron at Diamond Light Source.
It’s hard to convey the scale of the thing; turns out you need a big ol’ ring if you want to spin electrons fast enough to generate a meaningful amount of magnetobremsstrahlung
radiation.
The whole thing’s highly-recommended if you’re able to get to one of their open days in the future, give it a look. I was particularly pleased to see how enthused about science it made
the kids, and what clever questions they asked.
For example: the 7-year-old spent a long time cracking a variety of ciphers in the computing tent (and even spotted a flaw in one of the challenge questions that the exhibitors then had
to hand-correct on all their handouts!); the 10-year-old enjoyed quizzing a researcher who’d been using x-ray crystallography ofproteins.
Medicine
And then on Sunday I finally got a long-overdue visit to my nearest spirometry specialist for a suite of experiments to try to work out what exactly is wrong with my lungs, which
continue to be a minor medical mystery.
“Once you’ve got your breath back, let’s fill you with drugs and do those experiments again…”
It was… surprisingly knackering. Though perhaps that’s mostly because once I was full of drugs I felt briefly superpowered and went running around the grounds of the wonderfully-named
Brill Hill Windmill with the dog until was panting in pretty much the way that I might normally have been,
absent an unusually-high dose of medication.
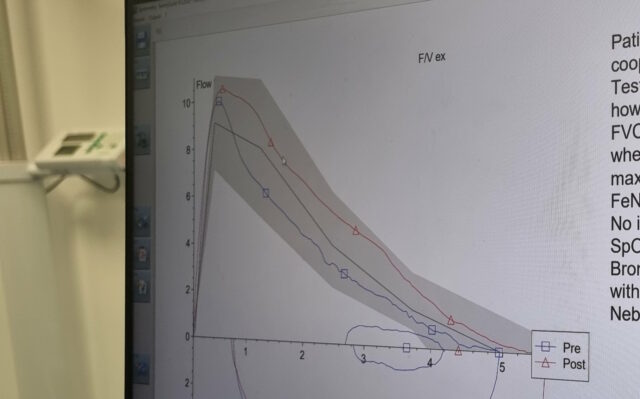
It’s got a graph; that makes it science, right? (I’m ignoring those party political histograms that outright lie about how narrow the margins are…)
For amusement purposes alone, I’d be more-likely to recommend the first day’s science activities than the second, but I can’t deny that it’s cool to collect a load of data about your
own body and how it works in a monitorable, replicable way. And maybe, just maybe, start to get to the bottom of why my breathing’s getting so much worse these last few years!
So the NHS blood donation rules are changing again. And while they’re certainly getting closer, they’re still not quite hitting the bullseye yet.
That’s great. Prior to 2011 men who’d ever had sex with men, as well as women who’d had sex with such a man within the last 6 months, were banned from donating blood. That rule
clearly spun out of the AIDS hysteria of the 1980s and generally entrenched homophobia. It probably did little to
protect the recipients of blood, and certainly did a lot to increase the stigma experienced by non-straight men.
You throw enough policies at a problem, eventually one will get close-enough, right?
The 2011 change permitted donation by men who’d previously had sex with men… so long as they hadn’t done so within the last year. Which opened the doors to donation by a lot of men:
e.g. bisexual men who’d been in relationships exclusively with women, gay men who’d been celibate for a period, etc. It still wasn’t great, but it was a step in the right
direction.
So when I saw that the rules were changing to better target only risky behaviours, rather than behaviours that are so broad-brush as to target identities, I was
initially delighted. Evidence-based medicine, you say? For the win.
Go on! Stick it in me! I’ll still be able to give blood, right?
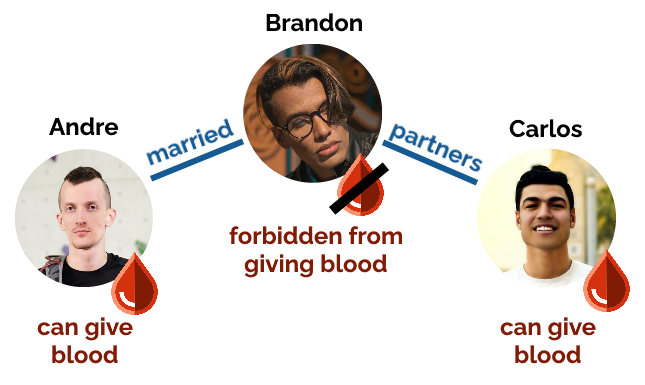
But… it’s not all sunshine and rainbows. The new rules prohibit blood donation regardless of gender by people who’ve had sex with more than one person in the last three months.
Sorry Brandon, we only want Andre and Carlos’ blood.
So if for example if there’s a V-shaped relationship consisting of three men, who only have sex within their thruple… two of them are now allowed to give blood but the third isn’t?
(This isn’t a contrived example. I know such a thruple.)
Stranger still: if you swap Brandon in the diagram above for a woman then you get a polycule that’s a lot like mine, but the woman in the middle used to be allowed to give
blood… and now can’t! My partner Ruth is in exactly the position: her situation hasn’t changed, but because she’s been in a long-term
relationship with exactly two people she’s now not allowed to give blood. Wot?
On the whole, this rule change is an improvement. We’re getting closer to a perfect answer. But it’s amusing to see where the policy misses again and excludes
donors who would otherwise be perfectly viable.
Update: as this is attracting a lot of attention I just wanted to remind people that the whole discussion is, of course, a lot
more complicated than can be summarised in a single, short, opinionated blog post. Take a look at the FAIR steering
group’s recommendations and compare to the government’s press release.
Update #2: justifying choice of words – “AIDS hysteria”
refers specifically to the media (and to a lesser extent the policy) reactions to the (very real, very devastating) pandemic. For a while there it was perfectly normal to see (often
misguided, sometimes homophobic) scaremongering news coverage suggesting that everybody was at enormous risk from HIV.
This is Lorcán. Lorcán has cystic fibrosis (CF) Lorcán is two years old. Lorcán has been fighting a potentially life shortening lung infection for the last six months and treatment
isn’t working.
There is an amazing drug called Orkambi made by Vertex that is not funded on the NHS, this drug could help Lorcán and thousands of others. Over 240 people in the U.K. have died
waiting for it to become available. Vertex and the U.K. government are letting people with CF die because of a disagreement over cost.
Parents have had to find an alternative way of getting these drugs for their children and the Cystic Fibrosis Buyers
Club have found a generic copy of the drug that individuals can legally import, it is a fifth of the cost. This is however still beyond what we can pay.
…
I’ve previously shared (one, two) content about my friend Jen‘s two-year-old son Lorcán, who suffers from cystic fibrosis, as well as joining in the
#strawfiechallenge earlier this year. A particular aim of Jen has been to get access to a drug that could add decades to her son’s life, but which isn’t being made available on the
NHS. Running out of options to get access to medicine that could dramatically improve her kid’s quality of life and prognosis,
she’s now set up a GoFundMe and is soliciting donations.
Parachute use did not reduce death or major traumatic injury when jumping from aircraft in the first randomized evaluation of this intervention.
However, the trial was only able to enroll participants on small stationary aircraft on the ground, suggesting cautious extrapolation to high altitude jumps.
…
As always, when the BMJ publish a less-serious paper, it’s knock-your-socks-off funny. In this one, a randomised trial to determine whether or not parachutes are effective (compared to
a placebo in the form of an empty backpack) at preventing death resulting from falling from an aircraft, when used by untrained participants, didn’t get many volunteer participants
(funny, that!) until the experiment was adapted to involve only a leap from a stationary, grounded aircraft with an average jump height of 0.6 metres.
That no one would ever jump out of an aeroplane without a parachute has often been used to argue that randomising people to either a potentially life saving medical intervention or a
control would be inappropriate, and that the efficacy of such an intervention should be discerned from clinical judgment alone. We disagree, for the most part. We believe that
randomisation is critical to evaluating the benefits and harms of the vast majority of modern therapies, most of which are unlikely to be nearly as effective at achieving their end
goal as parachutes are at preventing injury among people jumping from aircraft.
However, RCTs are vulnerable to pre-existing beliefs about standard of care, whether or not these beliefs are justified. Our attempts to recruit in-flight passengers to our ambitious
trial were first met with quizzical looks and incredulity, predictably followed by a firm, “No, I would not jump without a parachute.” For the majority of the screened
population of the PARACHUTE trial, there was no equipoise—parachutes are the prevailing standard of care. And we concur.
But what if we provided assurances that the planes were stationary and on the ground, and that the jump would be just a couple of feet? It was at this point that our study took off.
We set out in two groups, one at Katama Airfield on Martha’s Vineyard and the other at the Yankee Air Museum in Ann Arbor. One by one, our study subjects jumped from either a small
biplane or a helicopter, randomised to either a backpack equipped with a parachute or a look-a-like control. As promised, both aircraft were parked safely on terra firma. The matchup
was, unsurprisingly, a draw, with no injuries in either group. In the first ever RCT of parachutes, the topline conclusion was clear: parachutes did not reduce death or major
traumatic injury among people jumping from aircraft.
But topline results from RCTs often fail to reveal the full story. We conducted the PARACHUTE trial to illustrate the
perils of interpreting trials outside of context. When strong beliefs about the standard of care exist in the community, often only low risk patients are enrolled in a trial, which
can unsalvageably bias the results, akin to jumping from an aircraft without a parachute. Assuming that the findings of such a trial are generalisable to the broader population may
produce disastrous consequences.
Using humour to kickstart serious conversations and to provide an alternative way of looking at important research issues is admirable in itself.
Fantastic lightweight introduction to bacteriophages and how they can potentially be our next best weapon against infection as
we approach the post-antibiotic age. Plus an interesting look at the history and the discovery of bacteriophages!
Some 702 intimate examinations were done on sedated or anaesthetised patients (table 3). In only 24% of these examinations had written consent been obtained, and a further 24% of examinations were conducted apparently
without written or oral consent.
…
This 2003 study at an “English medical school” determined that vaginal/rectal examinations were routinely carried out on anaesthetised patients without their knowledge or consent. “I
was told in the second year that the best way to learn to do [rectal examinations] was when the patient was under anaesthetic,” one fourth year student responded, to the survey, “That
way they would never know.”
My friend Jen‘s been blogging and vlogging about cystic fibrosis – which her young son Lorcán has – in order to raise awareness of
it and of a promising new treatment, Orkambi, which would very likely dramatically improve the lifespan and health of chidren like Lorcán… were it available on the NHS. For more
information, including petitions you can sign, see their blog Little Fierce One.
Warning: this blog post contains pictures of urine, invasive equipment, and the inside of a bladder. It’s probably safe for all audiences, but you might like to put
your glass of apple juice down for a minute or two. The short of it all is that I’m probably healthy.
Since my hospitalisation the other month with a renal system infection, I’ve undergone a series of investigations to try to determine if
there’s an underlying reason that I fell ill. As my doctor explained to me, it’s quite possible that what I’d experienced was a random opportunistic infection (perhaps aided by
a course of unrelated antibiotics I’d been on earlier this year or by certain lifestyle habits), but if that wasn’t the case – if there were some deeper explanation for my health
problems – it was important to find out sooner, rather than later.
I’ve peed in so many little pots! If you laid them end-to-end across your kitchen counter, people would think that you were some kind of pervert.
Early on I had several ultrasound scans of my bladder (at a number of different times and at a variety of levels of fullness) and one of my kidneys, the latter of which revealed some
“minor scarring” of one of them which apparently isn’t something I should be worried about… although I wish they’d started the two-page letter I got with that rather than
opening with, effectively, “Contrary to what we told you at the hospital, we did later see something wrong with you…” But still, good to be reassured that this is probably not
an issue.
An ultrasound scan of one of my kidneys. Can you tell the sex yet?
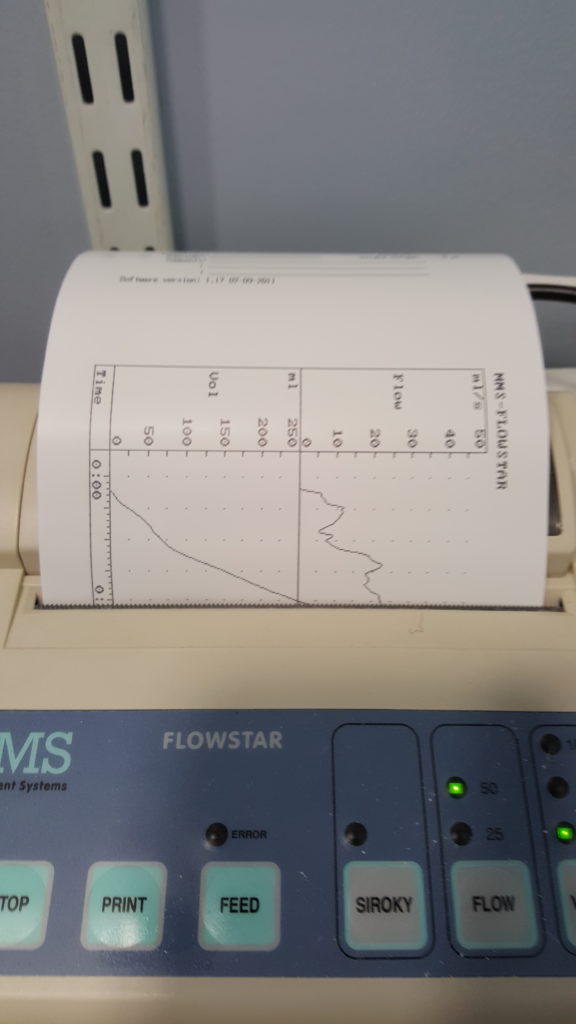
More recently, I went to the hospital to have a “flow rate test” and a cystoscopy. The flow rate test involved the most-ghetto looking piece of NHS equipment I’ve ever seen:
functionally, it seemed to be little more than a funnel on top of a large measuring beaker, in turn on top of a pressure-sensitive digital scale. The scale was connected up to the only
fancy-looking bit of equipment in the room, a graphing printer that output the calculated volume (based on their weight) of the same and, more-importantly, the rate of change: the “flow
rate” of the stream of urine.
I suppose one advantage of using equipment like this is that it basically operates itself. Which meant that the nurse was able to give me five seconds worth of instruction and then
leave the room, which saved us from our own Britishness forcing us to make small-talk while I urinated in front of her or something. Ultimately, I turned out to be within the range of
normalcy here, too, although I was a little disappointed to find that the ward didn’t maintain a daily “score board” of flow rates, as sort-of a science-backed literal pissing contest.
Apparently not all men experience that ‘spurt-and-then-full-pressure’ thing you’ll see on the graph on the right, when they start to pee, but some of us do, and it’s perfectly normal.
I’m learning so much!
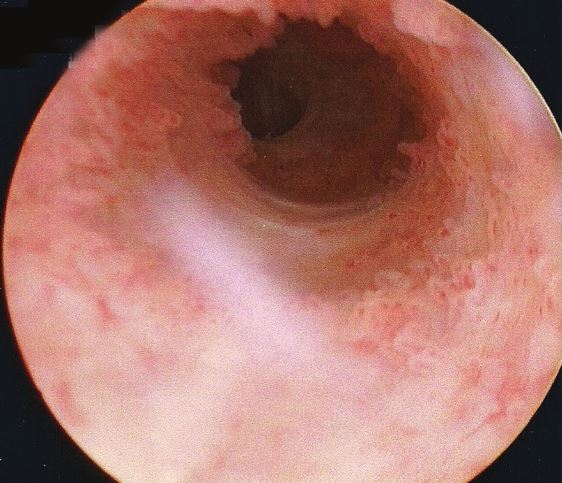
Finally came the cystoscopy, and this was the bit that I’d been most-nervous about. This procedure involves the insertion of a long flexible tube into the urethra at the tip of the
penis, under local anasthetic, and pushing it all the way down, through the sphincter, down through the prostate and then back up into the bladder. It’s then used as a channel to pump
water into the bladder, filling it to capacity and stretching out the sides, after which the fibreoptic cord (and light) that runs along its length is used to look around inside the
bladder to inspect for any of a plethora of different problems.
You’re going to put that WHERE?
The doctor invited me to watch with him on the monitor, which I initially assumed was because I was clearly interested in everything and kept asking questions, but in hindsight I wonder
if it’s just that he – quite rightly – assumed that I might have panicked if I’d have been looking in the direction of the piece of equipment he brought in and jabbed at my penis with.
I only looked at it while it was on its way out, and my god its a scary-looking thing: sort of like a cross between a tyre pressure gauge and a blowtorch. The first few inches were
painless – the local anasthetic had made me completely numb right up to and including the external sphincter, which is at the base of the penis. However, what I can only assume was the
second sphincter complained of the discomfort, and it stung pretty sharply any time the doctor would twist the cystoscope to change the angle of the picture.
The view as you ‘travel’ up the urethra looks pretty much like I expected. With a motion simulator, it would make a pretty cool ride!
Seeing the inside of your own body is an amazing experience. I mean: it’s not amazing enough to even be worth the experience of a cystoscopy, never mind the illness that in my case
preceeded it… but it’s still pretty cool. The ultrasounds were interesting, but there’s nothing quite so immersive as seeing a picture of the inside of your own bladder, gritting your
teeth while the doctor points to an indentation and explains that it’s the opening to the ureter that connects to your own left kidney!
Unfortunately I neglected to take my phone into the operating room, having put it into a locker when I changed into a gown, and so I wasn’t able to (as I’d hoped) take photos of the
inside of my own bladder. So you’ll have to make do with this video I found, which approximates the experience pretty well. The
good news is that there’s probably nothing wrong with me, now that the infection from earlier this year has passed: nothing to suggest that there’s any deeper underlying issue
that caused me to get sick, anyway!
The bad news is that while the procedure itself was shorter and more-bearable than I’d expected, the recovery’s been a real drag. A week later, it still hurts a lot to urinate (although
I’ve stopped yelping out loud when I do so) and my crotch is still too sore for me to be able to cycle. I’ve also discovered that an errection can be painful enough to wake me up, which
is definitely not the most-pleasant way I’ve been roused by a penis. But it’s getting better, day by day, and at least I know for sure that I’m more-or-less “right” in the renal system,
now.
As I mentioned last week, I’ve been ill. For those who wanted the grisly details, well: here you go.
Warning: this blog post contains frank subjective descriptions of the symptoms of slightly-icky medical conditions including photographs. It’s probably safe for all
audiences, but you might not want to be drinking anything while you read it.
The trouble began, I suppose, about a month and a half ago, when a contracted what seemed to be a minor urinary tract
infection. If you’re a woman then, statistically-speaking, I probably don’t need to tell you what that is, but for the benefit of the men: it’s what happens when bacteria (or,
sometimes, a fungus or virus) infects the renal system: the kidneys, bladder, ureters, and especially the urethra. It’s not pleasant: it gives you the feeling of needing to pee the
whole time, makes it harder to pee, and – when you do – it feels a little bit like you’re piss is made of lava.
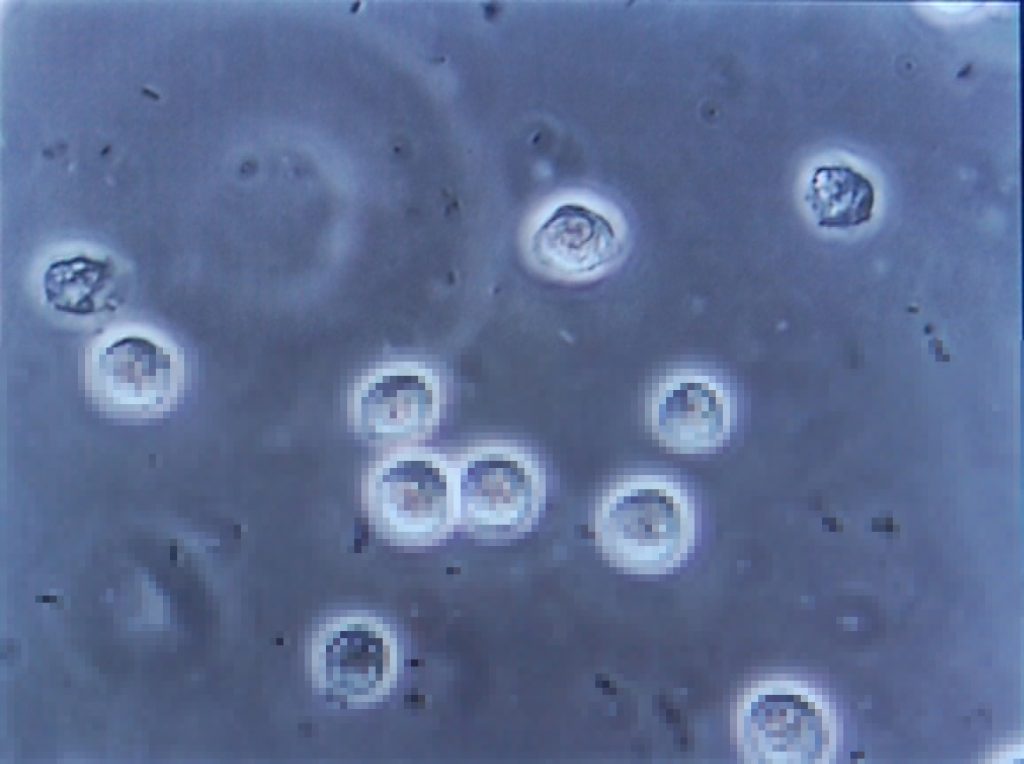
This urine contains white blood cells (the big circles) and bacteria (the tiny ‘wormlike’ things). Healthy urine contains little to none of these. Anybody else feel like they’re
playing Spore?
Despite it not being common for men (more on that later), I’ve had mild UTIs on a couple of occasions in my life, and I’d always found
that ensuring that I got plenty of water and a full RDA of vitamin C was more than enough to make it clear up all by itself
within a couple of days. So that’s what I started doing. But then things took a turn for the worse: I started getting a stabbing pain in my left kidney. Recognising this as being
pyelonephritis, I went to the doctor who prescribed me a course of the antibiotic ciprofloxacin. Within a couple of days I was
feeling right as rain (of course I continued to finish the course of drugs, although I was interested to see that that advice is
starting to become controversial).
Happy, healthy, and out for a picnic.
Naturally I was a little disappointed when, the week before last, I started getting UTI-like pain again, followed very swiftly
this time by pain in my bladder that constantly felt a little like I was recovering from being punched. Back to the doctor I went, where (after the usual tests to work out what the
most-likely best-antibiotic to use was) I was prescribed a course of nitrofurantoin. I’d never had this particular drug
before, and it wasn’t initially clear which of the escalating ill-effects I was experiencing were symptoms of the infection and which were side-effects of the medication: it started
with joint pain, then nausea, then diarrhoea, then a full-on fever. It was at the point that I was fully-clothed in bed, running a temperature and soaked in sweat but still feeling cold
and shivering that Ruth called 111, who told her to take me to A&E.
(Which, like her care for me in general, she did fabulously well, except for a little bit where she sort-of ran me over in the car park of the hospital: thankfully some
friendly paramedics were standing around and were able to drag me into the building. Anyway, I don’t have much memory of that bit and I certainly don’t have any amusing photos, so I’ll
skip over it.)
Feverish to the point of delirium, I don’t have much recollection of the first few hours(?) in the hospital. But I was alert enough to request that a photo was taken for the
inevitable blog post. Ruth, however, insisted upon waiting until I apparently looked a lot less like I was about to die: so here it is!
A few tests later, the medical staff seemed confident that what I was experiencing was not an allergic reaction to the antibiotic (however, I see that they still made a note of it as a
risk on my notes!) but was a progression of the infection, which seemed to have crossed over from the tissues of my renal system and into my bloodstream and was now generally causing
havoc by attacking the rest of my body. They hooked me up to a drip of an intravenous antibiotic and kept me stocked with painkillers, then sent me up to the urology ward and set me up
with a “bed” (urology mostly deals with outpatients, and so my ‘bed’ was actually a trolley, but they wanted to keep me close to the urologists in case of any complications).
It was only the following morning, with the delirium passed, that I realised that I was on the sixth floor. Looking out of my window, I could just make out the spires of the Bodleian
Library in the distance, so I dropped my coworkers an email to apologise for not being on my way there.
A consultant switched me to a week’s course of yet-another different antibiotic – co-amoxiclav – and recommended
keeping me in for another night. Now, I think that co-amoxiclav is a really interesting drug, so I’m going to be a bit of a nerd and tell you about that for a bit (I promise we’ll get
back to my health in a moment: if you don’t want the science bit, just scroll past the diagrams to the next photo).
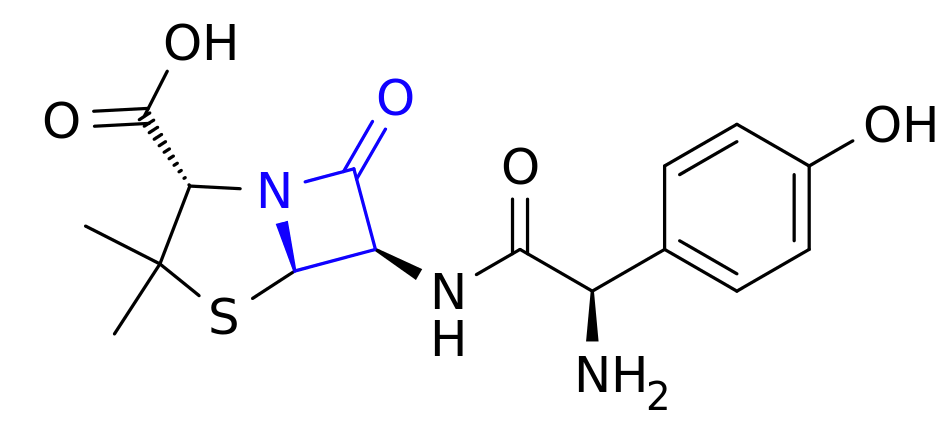
This is amoxicillin. I’ve highlighted in blue the lactam ring, which is the important bit.
Co-amoxiclav is a mixture of two drugs. The first is the antibiotic amoxicillin. Amoxicillin belongs to a class of antibiotics
(which includes penicillin) called β-lactams, which is the most-commonly used family of antibiotics. These antibiotics contain a four-point lactam ‘ring’ (highlighted in blue above),
and the way that they work is that this part of the molecule bonds with a particular protein common to all gram-positive
bacteria. Normally this protein is responsible for producing peptidoglycan, which is an essential ingredient in the cell walls
of these kinds of bacteria, but when it gets locked to a β-lactam ring it stops working. As a result, when the bacterium reproduces the new child doesn’t have a proper cell wall, and
can’t survive long in even the least-hostile environments.
Of course, we’re in a medical arms race right now because some of the bacteria which we’re targetting with antibiotics are becoming resistant. And here’s one what that they’re
doing so: some of these bacteria have evolved to produce beta-lactamase, also bonds with beta-lactam rings, adding an
OH to them and making them useless. Bummer, eh?
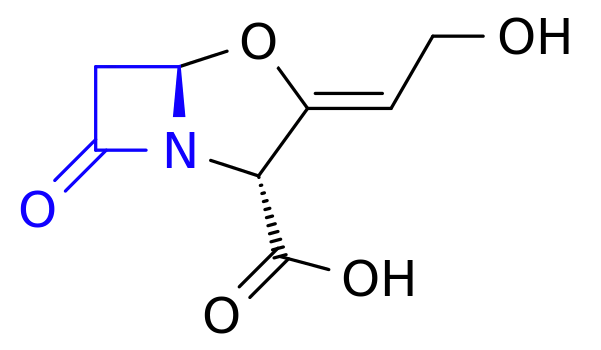
And this is clavulanic acid. Recognise that shape on the left-hand side of the molecule (highlighted in blue)? Yup: it’s another lactam ring.
The second drug in co-amoxiclav, then, is clavulanic acid, which was discovered in the 1970s and started being added to drugs
in the 1980s. Despite having a β-lactam ring (as you’ll see in blue above), clavulanic acid by itself it isn’t an effective antibiotic (for reasons I can’t quite get my head
around – anyone want to help me?). But what it’s great at is bonding that lactam ring to beta-lactamase, thereby deactivating the bacterial counter-offensive and allowing the
amoxicillin to carry on working, combating resistance.
So what you’ve got in co-amoxiclav is a an antibiotic and a chemical that counteracts the effects of a chemical that deactivates that antibiotic. Wow! It’s things like this
that really make me wish I had a brain for biology!
These things aren’t terribly comfortable when you’re trying to sleep.
I was eventually discharged from hospital and released to go home for lots of bed rest and water, along with a further week’s course of co-amoxiclav. Unfortunately it turns out that I’m
one of the unlucky folks for whom amoxicillin makes me dizzy, so I spent most of that week lying down in-between wobbly vertigo-filled trips to and from the bathroom. But it worked!
Within a few days I was feeling much better and by the end of last week I was able to work from home (and actually feel like I was useful again!).
Free of symptoms and off the drugs, I returned to work properly on Monday morning and everything seemed fine. Until, late in the morning, I went to the bathroom and started pissing
blood.
I took a picture, but it’s too grim even for this blog post. Here, have a kitten instead. Do an image search for ‘gross haematuria’ if you want a clue: the kitten will still be
waiting here when you need it.
Now apparently blood in your urine, while horrifying when it happens to you unexpectedly, isn’t actually a
sign of a medical emergency. I was starting to get bladder pain again, quite intensely, so I excused myself from work and called the urology ward, who decided that I wasn’t in bad
enough a condition to go and see them but sent me straight to my GP, who gave me another fortnight’s worth of co-amoxiclav. They’re monitoring my progress with urine and blood samples
and if by Friday it’s not having an impact, they’re going to want to send me back to hospital (hopefully only as an outpatient) and pump me full of the intravenous stuff again. So…
fingers crossed for a good result out of these drugs.
My co-amoxiclav tablets each come individually wrapped in a nitrogen-filled foil bag. I’ve no idea what it is that they’re concerned that they’ll react with, but I’m eating three of
them a day anyway.
I was hoping that by this point I’d be writing this blog post and telling you all about how I’d fought the bladder monster and won. But it looks like I won’t be able to claim that
victory for another week or two, yet. All I know is that I searched for “bladder monster” and found
this. Yeah: that feels about right.
A week ago, Ruth pushed a baby out of her body, completely upstaging my birthday and, incidentally,
throwing all of our lives pretty much into chaos. Having gotten to the point at which she’d resigned herself to “being pregnant forever“, Ruth would have certainly been glad to have that stage over and done with, were it not for a long and painful labour followed by
a torturous and exhausting birth.
If Ruth looks like she’s about to die of exhaustion in this photo, that’s because that’s how she’s feeling.
There’s a lot that can be said about the labour: a 38-hour crescendo of Ruth gradually and repeatedly finding levels of pain and tiredness that each seemed impossible, until she reached
them. But Ruth has suggested that she might like to write a little about it herself, so I shan’t steal her limelight. What I can say is that I didn’t – and I don’t think that JTA, either – appreciate quite how emotionally draining the experience would be for the two of us, as well. There was a
strange sensation for me about twelve hours in: a sensation perhaps most-comprehensible by our friends who’ve done emotional support work. That was: after watching somebody I love so
much suffer so greatly for so long, I felt as if I’d somehow begun to exhaust whatever part of my brain feels empathy. As if the experience of supporting Ruth had served to drain me in
a way I’d never fully experienced before, like when you discover a muscle you didn’t know you had when it aches after an unusual new exercise.
Forcep-marks still visible, the newborn takes an extended nap in a crib alongside Ruth’s recovery-bed.
Of course, after the ordeal we got to take home a little bundle of joy, who continues – despite now having a perfectly fabulous name of her own – to be referred to as “tiny”, even
though her birth weight of 8lbs 12oz (that’s about 4kg, for those who – like me – prefer to think in metric) doesn’t really make that a very fitting nickname! Nor the amount of damage
she did to Ruth on the way out, which also might be ill-described as “tiny”! She’s also often referred to as “the poopmachine”, for reasons that ought not need spelling out.
I’m smiling, because I don’t yet know that, within seconds of this photo being taken, she’s about to fill her nappy.
My employer was kind enough to give me paternity leave, even though I’m not the biological father (JTA is; and he’s very-much still in the picture!). I’d looked at my contract and
discovered that the wording seemed to imply that I was eligible, stating that I’d be permitted to take paternity leave if I was about to become a father, or if my partner was about to
give birth, the latter of which seemed perfectly clear. To be certain, I’d wandered along to Personnel and explained our living arrangement, and they just had looks on their faces that
said “we’re not touching that with a barge pole; let’s just err on the side of giving him leave!” As a result, we’ve had all hands on deck to help out with the
multitudinous tasks that have suddenly been added to our lives, which has been incredibly useful, especially given that Ruth has been spending several days mostly lying-down, as she’s
been recovering from injuries sustained during the delivery.
If only we had some kind of way to set up a web-based rota of feeding, changing and comforting the little one…
Despite everything, we and the rest of the Three Rings team still managed to push the latest version into testing on schedule, though
fitting in time for bug-fixing is even harder than it would be were we at our “day jobs” during the daytimes! It’s not that our little poopmachine takes up all of our time, though she
does seem to take a lot of it, it’s simply that we’re all so tired! For the last few nights she’s been fussy about sleeping, and we’ve all lost a lot of rest time over keeping her fed,
clean, and feeling loved.
Who loves boob? Baby does! Also, everybody else in the house.
For all my complaining, though, what we’ve got here is an adorable and mostly well-behaved little bundle of joy. And when she’s not covered in poop, shouting for
attention, or spitting milk all over you, she’s a little angel. And I’m sure you’ll all be sick of hearing about her very soon.
This is the first in a series of four blog posts which ought to have been published during January 2013,
but ran late because I didn’t want to publish any of them before the first one.
2012 was one of the hardest years of my life.
My retweet of JTA’s sentiments, shortly after midnight on New Year’s Eve, pretty much covers my feeling of the year, too.
It was a year of unceasing disasters and difficulties: every time some tragedy had befallen me, my friends, or family, some additional calamity was lined-up to follow in its wake. In an
environment like this, even the not-quite-so-sad things – like the death of Puddles, our family dog, in May – were magnified, and the ongoing challenges of the year – like the
neverending difficulties with my dad’s estate – became overwhelming.
My sister Becky with Puddles, both younger and more-foolish than they eventually became. I don’t know why Puddles is wearing a t-shirt.
The sudden and unexpected death of my dad while training for his Arctic trek, was clearly the event which had the most-significant impact on me.
I’ve written about the experience at length, both here on my
blog and elsewhere (for example, I made a self-post to Reddit on the day after the accident, urging readers to “call somebody you love today”).
My dad, climbing Aladdin’s Mirror in the Cairngorms.
In the week of his death, my sister Becky was suffering from an awful toothache which was stopping her from eating,
sleeping, or generally functioning at all (I tried to help her out by offering some oil of cloves (which functions as a dental contact anesthetic), but she must have misunderstood my instruction about applying it to the tooth
without swallowing it, because she spent most of that evening throwing up (seriously: don’t ever swallow clove oil).
My dad’s clothes for his funeral. My sisters and I decided that he ought to be dressed as he would be for a one of his summer hikes, right down to the combination of sandals and socks
(the funeral director needed reassurance that yes, he really did routinely wear both at the same time).
Little did she know, worse was yet to come: when she finally went to the dentist, he botched her operation,
leaving her with a jaw infection. The infection spread, causing septicæmia of her face and neck and requiring that she was hospitalised. On the day of our dad’s funeral, she needed to insist that the “stop gap” surgery that she was given was done under local, rather than general,
anasthetic, so that she could make it – albeit in a wheelchair and unable to talk – to the funeral.
Five weeks later, my dad finally reached the North Pole,
his ashes carried by another member of his team. At about the same time, Ruth‘s grandmother passed away, swamping the
already-emotional Earthlings with yet another sad period. That same month,
my friend S****** suffered a serious injury, a traumatic and distressing experience in the middle of a long and difficult period of her life, and an event which caused significant
ripples in the lives of her circle of friends.
The notice of Ruth’s grandmother’s death, as it appeared in the online version of her local newspaper.
Shortly afterwards, Paul moved out from Earth, in a situation that was anticipated (we’d said when we first moved in
together that it would be only for a couple of years, while we all found our feet in Oxford and decided on what we’d be doing next, as far as our living situations were concerned), but
still felt occasionally hostile: when Paul left town six months later, his last blog post stated that Oxford could “get lost”, and that he’d “hated hated 90% of the time” he’d lived here. Despite
reassurances to the contrary, it was sometimes hard – especially in such a difficult year – to think that this message wasn’t directed at Oxford so much as at his friends there.
As the summer came to an end, my workload on my various courses increased dramatically, stretching into my so-called “free time”: this, coupled with delays resulting from all of the
illness, injury, and death that had happened already, threw back the release date of Milestone: Jethrik, the latest update to Three Rings. Coupled with the stress of the 10th Birthday Party Conference – which thankfully JTA handled most of – even the rare periods during which nobody was ill or dying were filled with sleepless nights and anxiety. And of course as soon
as all of the preparation was out of the way and the conference
was done, there were still plenty of long days ahead, catching up on
everything that had been temporarily put on the back burner.
My sister Sarah and I at the christening of a bus named after my dad. Click the picture for the full story.
When I was first appointed executor of my dad’s estate, I said to
myself that I could have the whole thing wrapped-up and resolved within six months… eight on the outside. But as things dragged on – it took almost six months until the investigation
was finished and the coroner’s report filed, so we could get a death
certificate, for example – they just got more and more bogged-down. Problems with my dad’s will made it harder than expected to get started (for example, I’m the
executor and a beneficiary of the will, yet nowhere on it am I directly mentioned by name, address, or relationship… which means that I’ve had to prove that I am the person
mentioned in the will every single time I present it, and that’s not always easy!), and further administrative hiccups have slowed down the process every step of the way.
On the first anniversary of my dad’s death, I cycled up a hill to watch the sunset with a bottle of Guinness and a Mars bar. And sent this Tweet.
You know what would have made the whole thing easier? A bacon sandwich. And black
pudding for breakfast. And a nice big bit of freshly-battered cod. And some roast chicken. I found that 2012 was a harder year than 2011 in which to be a vegetarian. I guess that a nice steak would
have taken the edge off: a little bit of a luxury, and some escapism. Instead, I probably drank a lot more than I ought to have. Perhaps we should encourage recovering alcoholic, when
things are tough, to hit the sausage instead of the bottle.
It’s been a while, old friend. A while since I used this delicious-looking photograph in my blog, I mean! This is the sixth time… can you find them all?
Becky’s health problems weren’t done for the year, after she started getting incredibly intense and painful headaches. At first, I was worried that she was lined-up for a similar diagnosis to mine, of the other year (luckily, I’ve been symptom-free for a year
and a quarter now, although medical science is at a loss to explain why), but as I heard more about her symptoms, I became convinced that this wasn’t the case. In any case, she found
herself back in the operating room, for the second serious bit of surgery of the year (the operation was a success, thankfully).
The “F” is for “Fuck me you’re going to put a scalpel WHERE?”
I had my own surgery, of course, when I had a vasectomy; something I’d been
planning for some time. That actually went quite well, at least as far as can be
ascertained at this point (part three of that series of posts will be coming soon), but it allows me to segue into the topic of reproduction…
Because while I’d been waiting to get snipped, Ruth and JTA had managed to conceive. We found this out right as we were running around sorting out the Three Rings Conference, and Ruth
took to calling the fœtus “Jethrik”, after the Three Rings milestone. I was even more delighted still when I heard that the expected birth date would be 24th July: Samaritans‘ Annual Awareness Day (“24/7”).
One of the many pregnancy tests Ruth took, “just to be sure” (in case the last few were false positives). Photo from Ruth’s blog.
As potential prospective parents, they did everything right. Ruth stuck strictly to a perfectly balanced diet for her stage of pregnancy; they told only a minimum of people, because –
as everybody knows – the first trimester’s the riskiest period. I remember when Ruth told her grandfather (who had become very unwell towards the end of 2012 and died early this year:
another sad family tragedy) about the pregnancy, that it was only after careful consideration – balancing how nice it would be for him to know that the next generation of his
family was on the way before his death – that she went ahead and did so. And as the end of the first trimester, and the end of the year, approached, I genuinely believed that the string
of bad luck that had been 2012 was over.
In Ruth’s blog post, she’s used kittens to make a sad story a little softer, and so I have too.
But it wasn’t to be. Just as soon as we were looking forward to New Year, and planning to not so much “see in 2013” as to “kick out 2012”, Ruth had a little bleeding. Swiftly followed
by abdominal cramps. She spent most of New Year’s Eve at the hospital, where they’d determined that she’d suffered a miscarriage, probably a few weeks earlier.
Ruth’s written about it. JTA’s written about it, too. And I’d recommend they read
their account rather than mine: they’ve both written more, and better, about the subject than I could. But I shan’t pretend that it wasn’t hard: in truth, it was heartbreaking. At the
times that I could persuade myself that my grief was “acceptable” (and that I shouldn’t be, say, looking after Ruth), I cried a lot. For me, “Jethrik” represented a happy ending to a
miserable year: some good news at last for the people I was closest to. Perhaps, then, I attached too much importance to it, but it seemed inconceivable to me – no pun intended – that
for all of the effort they’d put in, that things wouldn’t just go perfectly. For me, it was all connected: Ruth wasn’t pregnant by me, but I still found myself wishing that my dad could
have lived to have seen it, and when the pregnancy went wrong, it made me realise how much I’d been pinning on it.
I don’t have a positive pick-me-up line to put here. But it feels like I should.
A few days before the miscarriage became apparent, Ruth and her dad survey the back garden of the house he’s rebuilding.
And so there we were, at the tail of 2012: the year that began awfully, ended awfully, and was pretty awful in the middle. I can’t say there weren’t good bits, but they were somewhat
drowned out by all of the shit that happened. Fuck off, 2012.
Here’s to 2013.
Edit, 16th March 2013: By Becky’s request, removed an unflattering photo of her and some of the ickier details of her health problems this year.
Edit, 11th July 2016: At her request, my friend S******’s personal details have been obfuscated in this post so that they are no longer readily available to
search engines.
Edit, 26th September 2016: At her request, my friend S******’s photo was removed from this post, too.




 Levelled up my blood donation game!
Levelled up my blood donation game!