Over the last three or four years I’ve undertaken a couple of different rounds of psychotherapy. I liken the experience to that of spotting constellations in the night sky.
That’s probably the result of the goal I stated when going in to the first round: I’d like you to help while I take myself apart, try to understand how I work, and then put myself
back together again.1I’m trying to connect the dots between who-I-once-was and who-I-am-now and find causal influences.
As I’m sure you can imagine: with an opening statement like that I needed to contact a few different therapists before I found one who was compatible with my aims2.
But then, I was always taught to get three quotes before hiring a professional.
Constellations are necessarily subjective. It’s always pleased me to think about how Orion the Hunter, one of the Northern hemisphere’s most-recognisable Winter visitors, was
interpreted by the Lakota people to represent a bison, and some Indian traditions see it as a deer.
It’s that “connecting the dots” that feels like constellation-spotting. A lot of the counselling work (and the “homework” that came afterwards) has stemmed from ideas like:
This star represents a moment in my past.
This star represents a facet of my identity today.
If we draw a line from one to the other, what does the resulting constellation look like?
I suppose that what I’ve been doing is using the lens of retrospection to ask: “Hey, why am I like this? Is this part of it? And what impact did that have on
me? Why can’t I see it?”
When you’re stargazing, sometimes you have to ask somebody to point out the shape in front of you before you can see it for yourself.
A better writer would make an allusion to looking into one’s past through the symbolism of looking into the Universe’s past, but I’m not that writer.
I haven’t yet finished this self-analytical journey, but I’m in an extended “homework” phase where I’m finding my own way: joining the dots for myself. Once somebody’s helped you find
those constellations that mean something to you, it’s easier to pick them out when you stargaze alone.
Footnotes
1 To nobody’s surprise whatsoever, I can reveal that ever since I was a child I’ve enjoyed
taking things apart to understand how they work. I wasn’t always so good at putting them back together again, though. My first alarm clock died that way, as did countless small
clockwork and electronic toys.
2 I also used my introductory contact to lay out my counselling qualifications,
in case they were a barrier for a potential therapist, but it turns out this wasn’t as much of a barrier as the fact that I arrived with a concrete mandate.
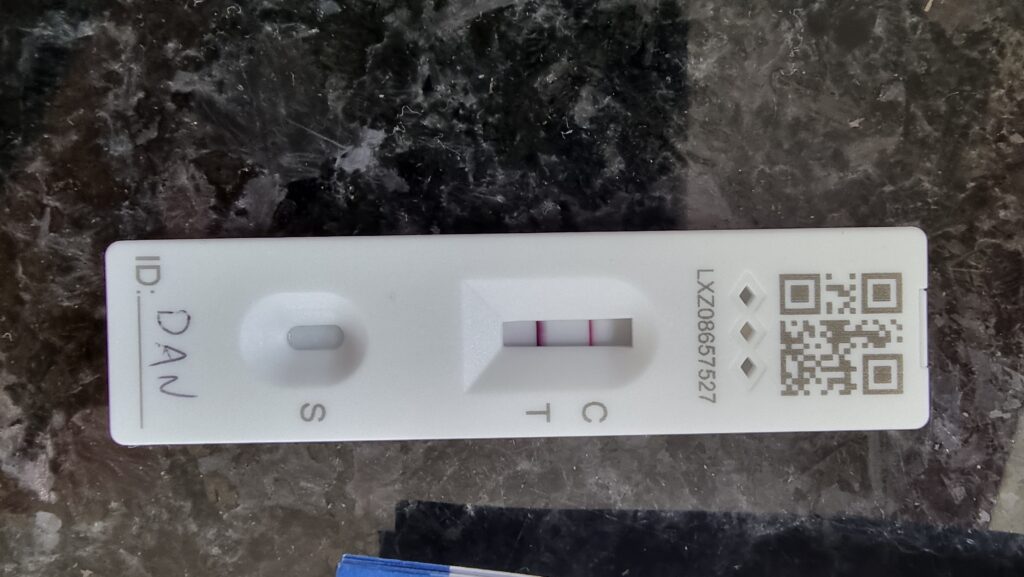
I managed to dodge infection for 922 days of the Covid pandemic1,
but it caught up with me eventually.
Well, shit.
Frankly, it’s surprising that it took this long. We’ve always been careful, in accordance with guidance at any given time, nd we all got our jabs and boosters as soon as we were able…
but conversely: we’ve got school-age children who naturally seem to be the biggest disease vectors imaginable. Our youngest, in fact, already had Covid, but the rest of us
managed to dodge it perhaps thanks to all these precautions.
The vaccine provide protection, but it’s not a magical force-field.
Luckily I’m not suffering too badly, probably thanks to the immunisation. It’s still not great, but I dread to think how it might have been without the benefit of the jab! A minor fever
came and went, and then it’s just been a few days of coughing, exhaustion, and… the most-incredible level of brain-fog.
Today, for example, I completey blanked the word “toilet” and struggled for some time to express to the dog why I’d brought her into the garden, while she stared at me expectantly.
I’ve taken the week off work to recover, which was a wise choice. As well as getting rest, it’s meant that I’ve managed to avoid writing production code with my addled brain! Instead,
I’ve spent a lot of time chilling in bed and watching all of the films that I’d been meaning to! This week, I’ve watched:
Peggy Sue Got Married (y’know, that other mid-1980s movie about time travel and being a teenager in the 1950s). It was okay; some bits of the direction were spectacular for its age,
like the “through the mirror” filming.
Fall. I enjoyed this more than I expected to. It’s not great, but while I spent most of the time complaining about the
lack of believability in the setting and the characters’ reactions, the acting was good and the tension “worked”: it was ocassionally pretty vertigo-inducing, and that’s not just
because I’ve been having some Covid-related dizziness!
RRR. Oh my god this Tollywood action spectacle was an adventure. At one point it’s a bromantic buddy comedy, then later
there’s a dance-off, then for a while there’s a wonderful “even language can’t divide us” romance, but then later a man picks up a motorcycle with one hand and uses it to beat up an
entire army, and somehow it all feels like it belongs together. The symbolism’s so thick you can spread it (tl;dr: colonialism
bad), but it’s still a riot of a film.
Cyrano, which I feel was under-rated but that could just be that I have a soft spot for the story… and a love of musical
theatre.
Also, at times when I didn’t think my brain had the focus for something new, I re-watched Dude, Where’s My Car? because
I figured a stoner comedy that re-replains the plot every 20 minutes or so was about as good as I could expect my brain to handle at the time, and Everything Everywhere All At Once which I’ve now seen three times and loved every single one: it’s one of my favourite films.
See, I’m fine! (Feel like I’ve spent a lot of time lying here, this week.)
Anyway: hopefully next week I’ll be feeling more normal and my poor Covid-struck brain can be trusted with code again. Until then: time to try to rest some more.
Footnotes
1 Based on the World Health Organisation’s declaration of the outbreak being a pandemic on
11 March 2020 and my positive test on 19 September 2022, I stayed uninfected for two years, six months, one week, and one day. But who’s counting?
I’ve been having a tough time these last few months. Thanks to COVID, I’m sure I’m not alone in that.
Times are strange, and even when you get a handle on how they’re strange they can still affect you: lockdown stress can quickly magnify anything else you’re already going
through.
We’ve all come up with our own coping strategies; here’s part of mine.
Only people who are highly-allergic to pine needles normally look like this when they’re shopping for a Christmas tree.
These last few months have occasionally seen me as emotionally low as… well, a particularly tough spell a decade ago. But this time around I’ve
benefited from the self-awareness and experience to put some solid self-care into practice!
By way partly of self-accountability and partly of sharing what works for me, let me tell you about the silly mnemonic that reminds me what I need to keep track of as part of each day:
GEMSAW! (With thanks to Amy Blankson for, among other things, the idea of this kind of acronym.)
Because it’s me, I’ve cited a few relevant academic sources for you in my summary, below:
Gratitude
Taking the time to stop and acknowledge the good things in your life, however small, is associated with lower stress levels (Taylor, Lyubomirsky & Stein, 2017) to a degree that can’t just be explained by the placebo effect (Cregg
& Cheavens, 2020).
Frankly, the placebo effect would be fine, but it’s nice to have my practice of trying to intentionally recognise something good in each day validated by the science too!
Exercise
I don’t even need a citation; I’m sure everybody knows that aerobic exercise is associated with reduced risk and severity of depression: the biggest problem comes from the
fact that it’s an exceptionally hard thing to motivate yourself to do if you’re already struggling mentally!
But it turns out you don’t need much to start to see the benefits (Josefsson, Lindwall & Archer,
2014): I try to do enough to elevate my heart rate each day, but that’s usually nothing more than elevating my desk to standing height, putting some headphones on, and dancing
while I work!
Warming up. Things only get nuts when the bass drops, but I’ll spare you having to watch that.
Meditation/Mindfulness
Understandably a bit fuzzier as a concept and tainted by being a “hip” concept. A short meditation break or mindfulness exercise might be verifiably therapeutic, but more
(non-terrible) studies are needed (Vonderlin, Biermann, Bohus & Lyssenko 2020). For me, a 2-5 minute
meditation break punctuates a day and feels like it contributes towards the goal of staying-sane-in-challenging-times, so it makes it into my wellbeing plan.
Maybe it’s doing nothing. But I’m not losing much time over it so I’m not worried.
Sunlight
During my 20s I gradually began to suffer more and more from “winter blues”. Nobody’s managed to make an argument for the underlying cause of seasonal affective disorder that
hasn’t been equally-well debunked by some other study. Small-scale studies often justify light therapy (e.g. Lam, Levitan & Morehouse 2006) but it’s possibly
no-more-effective than a placebo at scale (SBU 2007).
Since my early 30s, I’ve always felt better to get myself 30 minutes of lightbox on winter mornings (I use one of these bad
boys). I admit it’s possible that the benefits are just the result of tricking my brain into waking-up more promptly and therefore feeing like I’m being more-productive with my
waking hours! But either way, getting some sunlight – whether natural or artificial – makes me feel better, so it makes it onto my daily self-care checklist.
10 minutes of overhead, unoccluded sunlight is the minimum therapeutic dose. That translates to about 30 minutes of winter sun at my latitude or 10,000 lux full-spectrum sunlamp.
Acts of kindness
It’s probably not surprising that a person’s overall happiness correlates with their propensity for kindness (Lyubomirsky, King & Diener 2005). But what’s more interesting is that the causal link can be “gamed”. That is: a
deliberate effort to engage in acts of kindness results in increased happiness (Buchanan & Bardi
2010)!
Beneficial acts of kindness can be as little as taking the time to acknowledge somebody’s contribution or compliment somebody’s efforts. The amount of effort it takes is far
less-important for happiness than the novelty of the experience, so the type of kindness you show needs to be mixed-up a bit to get the best out of it. But demonstrating kindness
helps to make the world a better place for other humans, so it pays off even if you’re coming from a fully utilitarian perspective.
Writing
I write a lot anyway, often right here, and that’s very-definitely for my own benefit first and foremost. But off the back of
some valuable “writing therapy” (Baikie
& Wilhelm 2005) I undertook earlier this year, I’ve been continuing with the simpler, lighter approach of trying to no more than three sentences about something that’s had an
impact on me that day.
As an approach, it doesn’t help everybody (Zachariae 2015), but writing a little about your day – not even
about how you feel about it, just the facts will do (Koschwanez, Robinson, Beban, MacCormick, Hill, Windsor, Booth, Jüllig &
Broadbent 2017; fuck me that’s a lot of co-authors) – helps to keep you content, and I’m loving it.
Despite the catchy acronym (Do I need to come up with a GEMSAW logo?
I’m pretty sure real gemcutting is actually more of a grinding process…) and stack of references, I’m not actually writing a self-help book; it just sounds like I am.
I don’t claim to be an authority on anything beyond my own head, and I’m not very confident on that subject! I just wanted to share with you something that’s been working
pretty well at keeping me sane for the last month or two, just in case it’s of any use to you. These are challenging times; do what you need to find the happiness you can, and
hang in there.
This is Lorcán. Lorcán has cystic fibrosis (CF) Lorcán is two years old. Lorcán has been fighting a potentially life shortening lung infection for the last six months and treatment
isn’t working.
There is an amazing drug called Orkambi made by Vertex that is not funded on the NHS, this drug could help Lorcán and thousands of others. Over 240 people in the U.K. have died
waiting for it to become available. Vertex and the U.K. government are letting people with CF die because of a disagreement over cost.
Parents have had to find an alternative way of getting these drugs for their children and the Cystic Fibrosis Buyers
Club have found a generic copy of the drug that individuals can legally import, it is a fifth of the cost. This is however still beyond what we can pay.
…
I’ve previously shared (one, two) content about my friend Jen‘s two-year-old son Lorcán, who suffers from cystic fibrosis, as well as joining in the
#strawfiechallenge earlier this year. A particular aim of Jen has been to get access to a drug that could add decades to her son’s life, but which isn’t being made available on the
NHS. Running out of options to get access to medicine that could dramatically improve her kid’s quality of life and prognosis,
she’s now set up a GoFundMe and is soliciting donations.
#strawfiechallenge – 1 minute of simulated breathing difficulty in recognition of sufferers of cystis fibrosis
Today I’m attaching a clothes peg to my nose and breathing through a straw for 60 seconds. As I won’t be able to talk while I’m doing this, I’ll type an explanation why:
Like most people, I’ve spent most of my life lucky enough to not really know anything about cystic fibrosis. I first really became aware of it when my friend Jen‘s son Lorcán was diagnosed with it (you may remember I shared a video of hers
previously).
It’s a lifelong disorder with no known cure.
It’s a genetic disorder, and as many as one in every 25 people carries the gene that can cause it. Inherit two genes and you’re a sufferer. Among other symptoms, it causes frequent lung
infections and difficulty breathing.
I’m taking part in the #strawfiechallenge as an exercise in appreciating how difficult it can be to cope with reduced lung function. A new drug, Orkambi, is helping to extend the lives
of sufferers in other countries around the world. But it’s not yet available in the UK. :-(
CF sufferers want #OrkambiNow. They need your politicians to act.
Bitesize introduction to the (mostly-unspoken) history of the last century of sanitary products. It wasn’t so long ago – still within living memory! – that doctors’ advice was not to
exercise during your period and that sanitary products had to be packaged in plain containers so as not to embarrass buyers nor sales assistants. Humans have had a long and complicated relationship with menstruation but the largest and fastest period (no pun intended) of cultural
change has been only recently, and we now live in a world divided by a huge diversity of opinion and philosophy on the subject. This video covers only a fraction of the story of the
recent (Western) social change, but it’s still a strong reminder of how far we’ve come as a culture.
An increasing number of people are reportedly suffering from an allergy to the meat and other products of nonhuman mammals, reports Mosaic Science this week, and we’re increasingly confident that the cause is
a sensitivity to alpha-gal (Galactose-alpha-1,3-galactose), a carbohydrate produced in the bodies of virtually
all mammals except for us and our cousin apes, monkeys, and simians (and one of the reasons you can’t transplant tissue from pigs to humans, for example).
The lone star tick (You call that a star, tick? Looks like a blob to me!), one of several vectors for alpha-gal sensitivity.
The interesting thing is that the most-common cause of alpha-gal sensitivity appears to be the bite of one of a small number of species of tick. The most-likely hypothesis seems to be
that being bitten by such a tick after it’s bitten e.g. deer or cattle may introduce that species’ alpha-gal directly to your bloodstream. This exposure triggers an immune response
through all future exposure, even if it’s is more minor, e.g. consuming milk products or even skin contact with an animal.
That’s nuts, isn’t it? The Mosaic Science article describes the reaction of Tami McGraw, whose symptoms began in 2010:
[She] asked her doctor to order a little-known blood test that would show if her immune system was reacting to a component of mammal meat. The test result was so strongly positive,
her doctor called her at home to tell her to step away from the stove.
That should have been the end of her problems. Instead it launched her on an odyssey of discovering just how much mammal material is present in everyday life. One time, she took
capsules of liquid painkiller and woke up in the middle of the night, itching and covered in hives provoked by the drug’s gelatine covering.
When she bought an unfamiliar lip balm, the lanolin in it made her mouth peel and blister. She planned to spend an afternoon gardening, spreading fertiliser and planting flowers, but
passed out on the grass and had to be revived with an EpiPen. She had reacted to manure and bone meal that were enrichments in bagged compost she had bought.
Cats can eat bacon. But some cat owners can’t. More bacon for the cats? The plot thickens. Also: haven’t used this picture in
a while, have I?
Of course, this isn’t the only nor even the most-unusual (or most-severe) animal-induced allergy-to-a-different-animal we’re aware of. The hilariously-named but terribly-dangerous
Pork-Cat syndrome is caused, though we’re not sure how, by exposure to cats and
results in a severe allergy to pork. But what makes alpha-gal sensitivity really interesting is that it’s increasing in frequency at quite a dramatic rate. The culprit? Climate change.
Probably.
It’s impossible to talk to physicians encountering alpha-gal cases without hearing that something has changed to make the tick that transmits it more common – even though they don’t
know what that something might be.
…
“Climate change is likely playing a role in the northward expansion,” Ostfeld adds, but acknowledges that we don’t know what else could also be contributing.
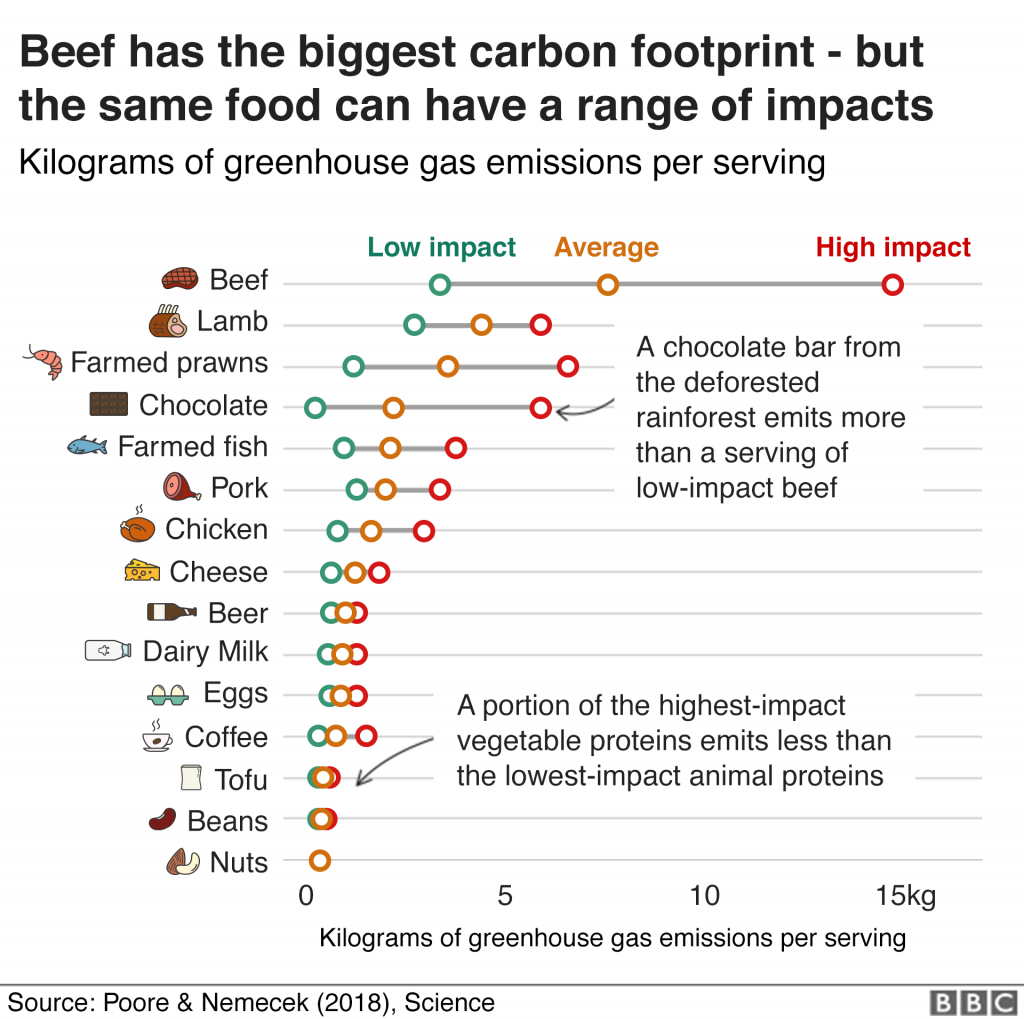
An average serving of beef contributes almost 8kg of greenhouse gases, compared to around 1kg for chicken. Thanks, Beeb (click through for full article).
A little dated, perhaps: I’m sure that nobody needs to be told nowadays that one of the biggest things a Westerner can do to reduce their personal carbon footprint (after from breeding less or not at all, which I maintain is the biggest, or avoiding air
travel, which Statto argues for) is to reduce or refrain from consumption of meat (especially pork and beef) and dairy products.
Indeed, environmental impact was the biggest factor in my vegetarianism (now weekday-vegetarianism) for
the last eight years, and it’s an outlook that I’ve seen continue to grow in others over the same period.
Seeing these two stories side-by-side in my RSS reader put the Gaia hypothesis in my mind.
If you want a pop-culture-grade introduction to the Gaia hypothesis in the context of climate change, this SMBC comic does the job, and does so almost with fewer words than this
caption explaining that it does so.
If you’re not familiar with the Gaia hypothesis, the basic idea is this: by some mechanism, the Earth and all of the life on it act in synergy to maintain homeostasis. Organisms not
only co-evolve with one another but also with the planet itself, affecting their environment in a way that in turn affects their future evolution in a perpetual symbiotic relationship
of life and its habitat.
Its advocates point to negative feedback loops in nature such as plankton blooms affecting the weather in ways that inhibit
plankton blooms and to simplistic theoretical models like the Daisyworld Simulation
(cute video). A minority of its proponents go a step further and describe the Earth’s changes teleologically, implying a conscious Earth with an intention to
protect its ecosystems (yes, these hypotheses were born out of the late 1960s, why do you ask?). Regardless, the essence is the same: life’s effect on its environment affects the
environment’s hospitality to life, and vice-versa.
There’s an attractive symmetry to it, isn’t there, in light of the growth in alpha-gal allergies? Like:
Today – climate change causes ticks to spread more-widely and bite more humans.
Tomorrow – tick bites cause humans to consume less products farmed from mammals?
Both my appreciation and my rejection of Gaia Hypothesis can probably be traced to me playing way too much SimEarth as a
teenager. Here’s my Daisyworld in state of equilibrium, because I haven’t yet gotten bored and spawned dinosaurs to eat all of the daisies.
That’s not to say that I buy it, mind. The Gaia hypothesis has a number of problems, and – almost as bad – it encourages a complacent “it’ll all be okay, the Earth will fix itself”
mindset to climate change (which, even if it’s true, doesn’t bode well for the humans residing on it).
But it was a fun parallel to land in my news reader this morning, so I thought I’d share it with you. And, by proxy, make you just a little bit warier of ticks than you might have been
already. /shudders/
My friend Jen‘s been blogging and vlogging about cystic fibrosis – which her young son Lorcán has – in order to raise awareness of
it and of a promising new treatment, Orkambi, which would very likely dramatically improve the lifespan and health of chidren like Lorcán… were it available on the NHS. For more
information, including petitions you can sign, see their blog Little Fierce One.
Warning: this blog post contains pictures of urine, invasive equipment, and the inside of a bladder. It’s probably safe for all audiences, but you might like to put
your glass of apple juice down for a minute or two. The short of it all is that I’m probably healthy.
Since my hospitalisation the other month with a renal system infection, I’ve undergone a series of investigations to try to determine if
there’s an underlying reason that I fell ill. As my doctor explained to me, it’s quite possible that what I’d experienced was a random opportunistic infection (perhaps aided by
a course of unrelated antibiotics I’d been on earlier this year or by certain lifestyle habits), but if that wasn’t the case – if there were some deeper explanation for my health
problems – it was important to find out sooner, rather than later.
I’ve peed in so many little pots! If you laid them end-to-end across your kitchen counter, people would think that you were some kind of pervert.
Early on I had several ultrasound scans of my bladder (at a number of different times and at a variety of levels of fullness) and one of my kidneys, the latter of which revealed some
“minor scarring” of one of them which apparently isn’t something I should be worried about… although I wish they’d started the two-page letter I got with that rather than
opening with, effectively, “Contrary to what we told you at the hospital, we did later see something wrong with you…” But still, good to be reassured that this is probably not
an issue.
An ultrasound scan of one of my kidneys. Can you tell the sex yet?
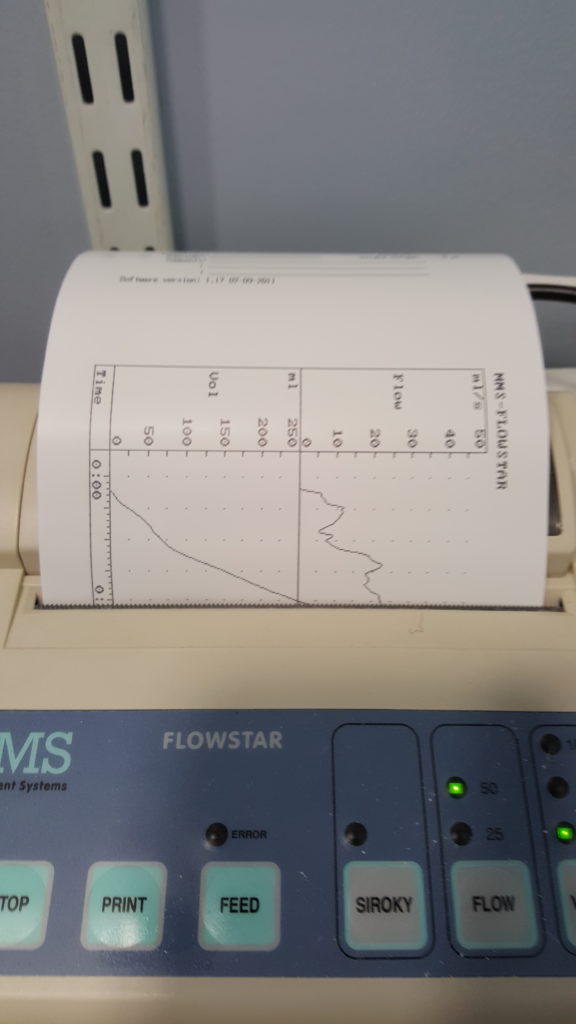
More recently, I went to the hospital to have a “flow rate test” and a cystoscopy. The flow rate test involved the most-ghetto looking piece of NHS equipment I’ve ever seen:
functionally, it seemed to be little more than a funnel on top of a large measuring beaker, in turn on top of a pressure-sensitive digital scale. The scale was connected up to the only
fancy-looking bit of equipment in the room, a graphing printer that output the calculated volume (based on their weight) of the same and, more-importantly, the rate of change: the “flow
rate” of the stream of urine.
I suppose one advantage of using equipment like this is that it basically operates itself. Which meant that the nurse was able to give me five seconds worth of instruction and then
leave the room, which saved us from our own Britishness forcing us to make small-talk while I urinated in front of her or something. Ultimately, I turned out to be within the range of
normalcy here, too, although I was a little disappointed to find that the ward didn’t maintain a daily “score board” of flow rates, as sort-of a science-backed literal pissing contest.
Apparently not all men experience that ‘spurt-and-then-full-pressure’ thing you’ll see on the graph on the right, when they start to pee, but some of us do, and it’s perfectly normal.
I’m learning so much!
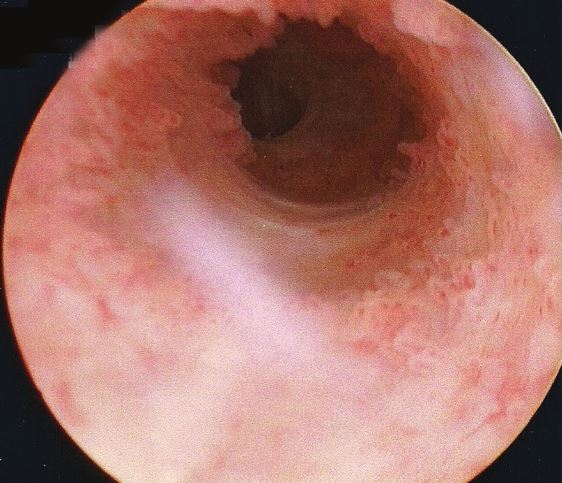
Finally came the cystoscopy, and this was the bit that I’d been most-nervous about. This procedure involves the insertion of a long flexible tube into the urethra at the tip of the
penis, under local anasthetic, and pushing it all the way down, through the sphincter, down through the prostate and then back up into the bladder. It’s then used as a channel to pump
water into the bladder, filling it to capacity and stretching out the sides, after which the fibreoptic cord (and light) that runs along its length is used to look around inside the
bladder to inspect for any of a plethora of different problems.
You’re going to put that WHERE?
The doctor invited me to watch with him on the monitor, which I initially assumed was because I was clearly interested in everything and kept asking questions, but in hindsight I wonder
if it’s just that he – quite rightly – assumed that I might have panicked if I’d have been looking in the direction of the piece of equipment he brought in and jabbed at my penis with.
I only looked at it while it was on its way out, and my god its a scary-looking thing: sort of like a cross between a tyre pressure gauge and a blowtorch. The first few inches were
painless – the local anasthetic had made me completely numb right up to and including the external sphincter, which is at the base of the penis. However, what I can only assume was the
second sphincter complained of the discomfort, and it stung pretty sharply any time the doctor would twist the cystoscope to change the angle of the picture.
The view as you ‘travel’ up the urethra looks pretty much like I expected. With a motion simulator, it would make a pretty cool ride!
Seeing the inside of your own body is an amazing experience. I mean: it’s not amazing enough to even be worth the experience of a cystoscopy, never mind the illness that in my case
preceeded it… but it’s still pretty cool. The ultrasounds were interesting, but there’s nothing quite so immersive as seeing a picture of the inside of your own bladder, gritting your
teeth while the doctor points to an indentation and explains that it’s the opening to the ureter that connects to your own left kidney!
Unfortunately I neglected to take my phone into the operating room, having put it into a locker when I changed into a gown, and so I wasn’t able to (as I’d hoped) take photos of the
inside of my own bladder. So you’ll have to make do with this video I found, which approximates the experience pretty well. The
good news is that there’s probably nothing wrong with me, now that the infection from earlier this year has passed: nothing to suggest that there’s any deeper underlying issue
that caused me to get sick, anyway!
The bad news is that while the procedure itself was shorter and more-bearable than I’d expected, the recovery’s been a real drag. A week later, it still hurts a lot to urinate (although
I’ve stopped yelping out loud when I do so) and my crotch is still too sore for me to be able to cycle. I’ve also discovered that an errection can be painful enough to wake me up, which
is definitely not the most-pleasant way I’ve been roused by a penis. But it’s getting better, day by day, and at least I know for sure that I’m more-or-less “right” in the renal system,
now.
As I mentioned last week, I’ve been ill. For those who wanted the grisly details, well: here you go.
Warning: this blog post contains frank subjective descriptions of the symptoms of slightly-icky medical conditions including photographs. It’s probably safe for all
audiences, but you might not want to be drinking anything while you read it.
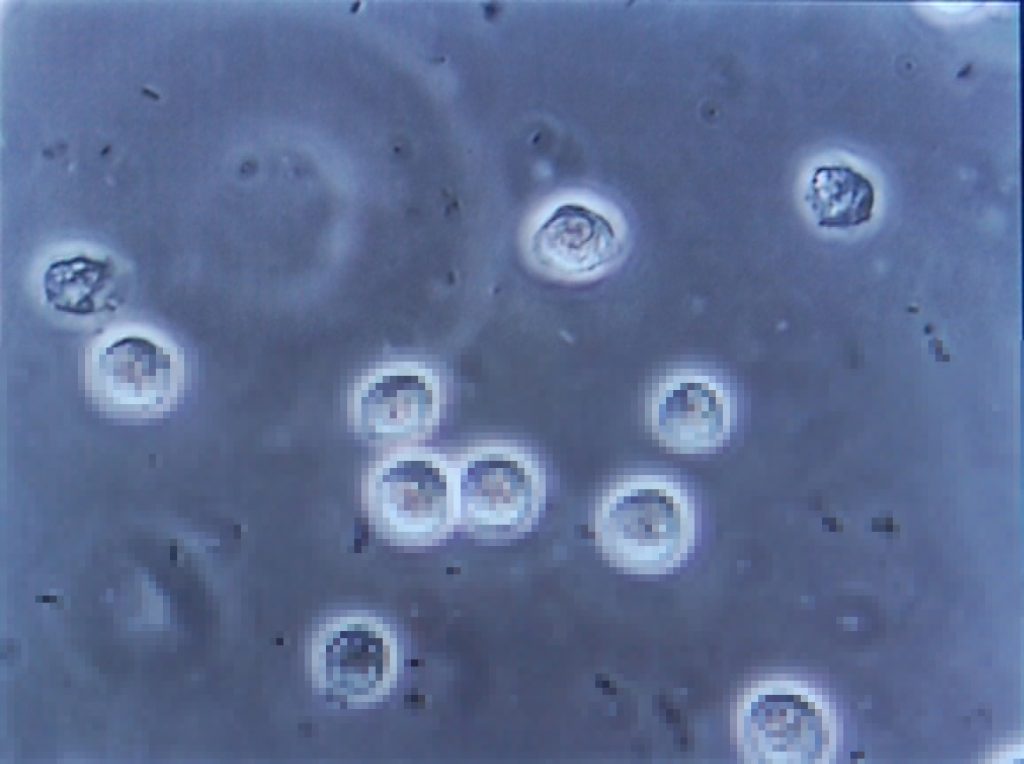
The trouble began, I suppose, about a month and a half ago, when a contracted what seemed to be a minor urinary tract
infection. If you’re a woman then, statistically-speaking, I probably don’t need to tell you what that is, but for the benefit of the men: it’s what happens when bacteria (or,
sometimes, a fungus or virus) infects the renal system: the kidneys, bladder, ureters, and especially the urethra. It’s not pleasant: it gives you the feeling of needing to pee the
whole time, makes it harder to pee, and – when you do – it feels a little bit like you’re piss is made of lava.
This urine contains white blood cells (the big circles) and bacteria (the tiny ‘wormlike’ things). Healthy urine contains little to none of these. Anybody else feel like they’re
playing Spore?
Despite it not being common for men (more on that later), I’ve had mild UTIs on a couple of occasions in my life, and I’d always found
that ensuring that I got plenty of water and a full RDA of vitamin C was more than enough to make it clear up all by itself
within a couple of days. So that’s what I started doing. But then things took a turn for the worse: I started getting a stabbing pain in my left kidney. Recognising this as being
pyelonephritis, I went to the doctor who prescribed me a course of the antibiotic ciprofloxacin. Within a couple of days I was
feeling right as rain (of course I continued to finish the course of drugs, although I was interested to see that that advice is
starting to become controversial).
Happy, healthy, and out for a picnic.
Naturally I was a little disappointed when, the week before last, I started getting UTI-like pain again, followed very swiftly
this time by pain in my bladder that constantly felt a little like I was recovering from being punched. Back to the doctor I went, where (after the usual tests to work out what the
most-likely best-antibiotic to use was) I was prescribed a course of nitrofurantoin. I’d never had this particular drug
before, and it wasn’t initially clear which of the escalating ill-effects I was experiencing were symptoms of the infection and which were side-effects of the medication: it started
with joint pain, then nausea, then diarrhoea, then a full-on fever. It was at the point that I was fully-clothed in bed, running a temperature and soaked in sweat but still feeling cold
and shivering that Ruth called 111, who told her to take me to A&E.
(Which, like her care for me in general, she did fabulously well, except for a little bit where she sort-of ran me over in the car park of the hospital: thankfully some
friendly paramedics were standing around and were able to drag me into the building. Anyway, I don’t have much memory of that bit and I certainly don’t have any amusing photos, so I’ll
skip over it.)
Feverish to the point of delirium, I don’t have much recollection of the first few hours(?) in the hospital. But I was alert enough to request that a photo was taken for the
inevitable blog post. Ruth, however, insisted upon waiting until I apparently looked a lot less like I was about to die: so here it is!
A few tests later, the medical staff seemed confident that what I was experiencing was not an allergic reaction to the antibiotic (however, I see that they still made a note of it as a
risk on my notes!) but was a progression of the infection, which seemed to have crossed over from the tissues of my renal system and into my bloodstream and was now generally causing
havoc by attacking the rest of my body. They hooked me up to a drip of an intravenous antibiotic and kept me stocked with painkillers, then sent me up to the urology ward and set me up
with a “bed” (urology mostly deals with outpatients, and so my ‘bed’ was actually a trolley, but they wanted to keep me close to the urologists in case of any complications).
It was only the following morning, with the delirium passed, that I realised that I was on the sixth floor. Looking out of my window, I could just make out the spires of the Bodleian
Library in the distance, so I dropped my coworkers an email to apologise for not being on my way there.
A consultant switched me to a week’s course of yet-another different antibiotic – co-amoxiclav – and recommended
keeping me in for another night. Now, I think that co-amoxiclav is a really interesting drug, so I’m going to be a bit of a nerd and tell you about that for a bit (I promise we’ll get
back to my health in a moment: if you don’t want the science bit, just scroll past the diagrams to the next photo).
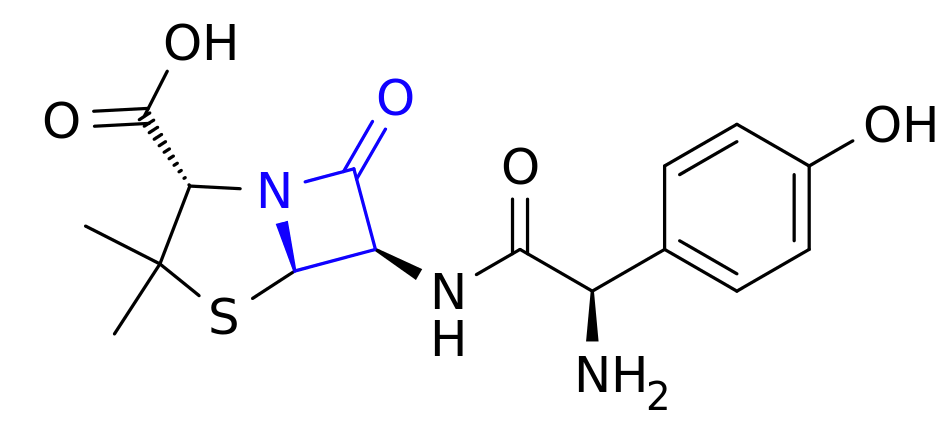
This is amoxicillin. I’ve highlighted in blue the lactam ring, which is the important bit.
Co-amoxiclav is a mixture of two drugs. The first is the antibiotic amoxicillin. Amoxicillin belongs to a class of antibiotics
(which includes penicillin) called β-lactams, which is the most-commonly used family of antibiotics. These antibiotics contain a four-point lactam ‘ring’ (highlighted in blue above),
and the way that they work is that this part of the molecule bonds with a particular protein common to all gram-positive
bacteria. Normally this protein is responsible for producing peptidoglycan, which is an essential ingredient in the cell walls
of these kinds of bacteria, but when it gets locked to a β-lactam ring it stops working. As a result, when the bacterium reproduces the new child doesn’t have a proper cell wall, and
can’t survive long in even the least-hostile environments.
Of course, we’re in a medical arms race right now because some of the bacteria which we’re targetting with antibiotics are becoming resistant. And here’s one what that they’re
doing so: some of these bacteria have evolved to produce beta-lactamase, also bonds with beta-lactam rings, adding an
OH to them and making them useless. Bummer, eh?
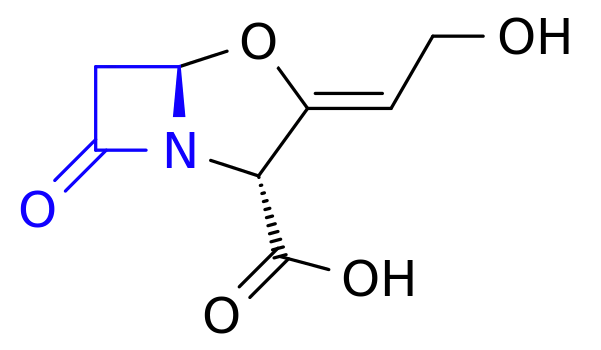
And this is clavulanic acid. Recognise that shape on the left-hand side of the molecule (highlighted in blue)? Yup: it’s another lactam ring.
The second drug in co-amoxiclav, then, is clavulanic acid, which was discovered in the 1970s and started being added to drugs
in the 1980s. Despite having a β-lactam ring (as you’ll see in blue above), clavulanic acid by itself it isn’t an effective antibiotic (for reasons I can’t quite get my head
around – anyone want to help me?). But what it’s great at is bonding that lactam ring to beta-lactamase, thereby deactivating the bacterial counter-offensive and allowing the
amoxicillin to carry on working, combating resistance.
So what you’ve got in co-amoxiclav is a an antibiotic and a chemical that counteracts the effects of a chemical that deactivates that antibiotic. Wow! It’s things like this
that really make me wish I had a brain for biology!
These things aren’t terribly comfortable when you’re trying to sleep.
I was eventually discharged from hospital and released to go home for lots of bed rest and water, along with a further week’s course of co-amoxiclav. Unfortunately it turns out that I’m
one of the unlucky folks for whom amoxicillin makes me dizzy, so I spent most of that week lying down in-between wobbly vertigo-filled trips to and from the bathroom. But it worked!
Within a few days I was feeling much better and by the end of last week I was able to work from home (and actually feel like I was useful again!).
Free of symptoms and off the drugs, I returned to work properly on Monday morning and everything seemed fine. Until, late in the morning, I went to the bathroom and started pissing
blood.
I took a picture, but it’s too grim even for this blog post. Here, have a kitten instead. Do an image search for ‘gross haematuria’ if you want a clue: the kitten will still be
waiting here when you need it.
Now apparently blood in your urine, while horrifying when it happens to you unexpectedly, isn’t actually a
sign of a medical emergency. I was starting to get bladder pain again, quite intensely, so I excused myself from work and called the urology ward, who decided that I wasn’t in bad
enough a condition to go and see them but sent me straight to my GP, who gave me another fortnight’s worth of co-amoxiclav. They’re monitoring my progress with urine and blood samples
and if by Friday it’s not having an impact, they’re going to want to send me back to hospital (hopefully only as an outpatient) and pump me full of the intravenous stuff again. So…
fingers crossed for a good result out of these drugs.
My co-amoxiclav tablets each come individually wrapped in a nitrogen-filled foil bag. I’ve no idea what it is that they’re concerned that they’ll react with, but I’m eating three of
them a day anyway.
I was hoping that by this point I’d be writing this blog post and telling you all about how I’d fought the bladder monster and won. But it looks like I won’t be able to claim that
victory for another week or two, yet. All I know is that I searched for “bladder monster” and found
this. Yeah: that feels about right.
So, I’ve not been well lately. And because a few days lying on my back with insufficient mental stimulation is a quick route to insanity for me, I’ve been trying to spend my
most-conscious moment doing things that keep my brain ticking over. And that’s how I ended up calculating pi.
When I say I’ve been unwell, that might be an understatement. But we’ll get to that another time.
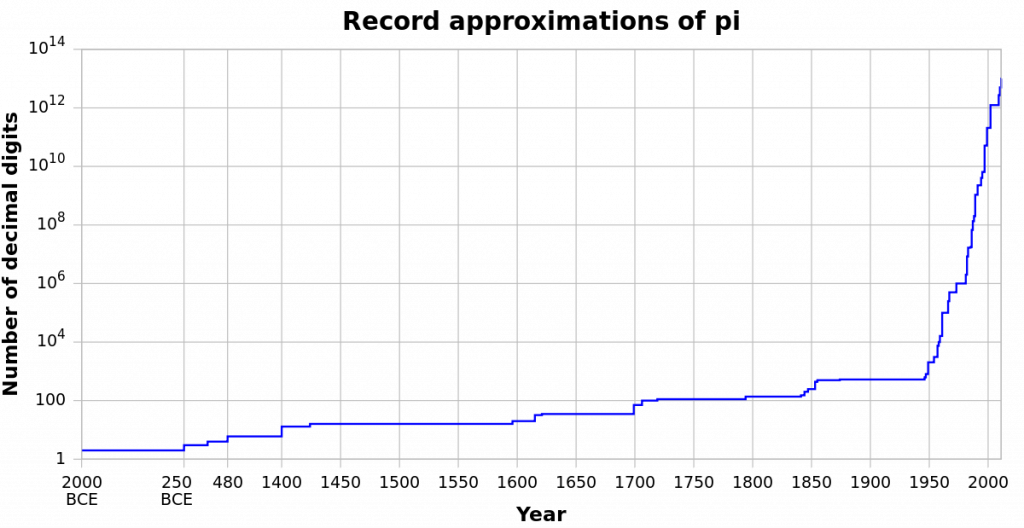
Pi (or π) is, of course, the ratio of the circumference of a circle to its diameter, for every circle. You’ll probably have learned it in school as 3.14, 3.142, or 3.14159, unless you
were one of those creepy kids who tried to memorise a lot more digits. Over the years, we’ve been able to calculate it to increasing precision, and although there’s no practical or theoretical reason that we need to know it beyond the 32 digits worked out by
Ludolph van Ceulen in the 16th Century, it’s still a fascinating topic that attracts research and debate.
Our calculation of pi has rocketed since the development of the digital computer.
Most of the computer-based systems we use today are hard to explain, but there’s a really fun computer-based
experimental method that can be used to estimate the value of pi that I’m going to share with you. As I’ve been stuck in bed (and often asleep) for the last few days, I’ve not
been able to do much productive work, but I have found myself able to implement an example of how to calculate pi. Recovery like a nerd, am I right?
Pi goes on forever. Pie, sadly, comes to an end.
Remember in school, when you’ll have learned that the formula to describe a circle (of radius 1) on a cartesian coordinate system is x2 + y2 = 1? Well you can work
this backwards, too: if you have a point on a grid, (x,y), then you can tell whether it’s inside or outside that circle. If x2 + y2 < 1, it’s inside, and if
x2 + y2 > 1, it’s outside. Meanwhile, the difference between the area of a circle and the area of a square that exactly contains it is π/4.
Think back to your school days. Ever draw a circle like this? Do the words “Cartesian coordinates” ring any bells?
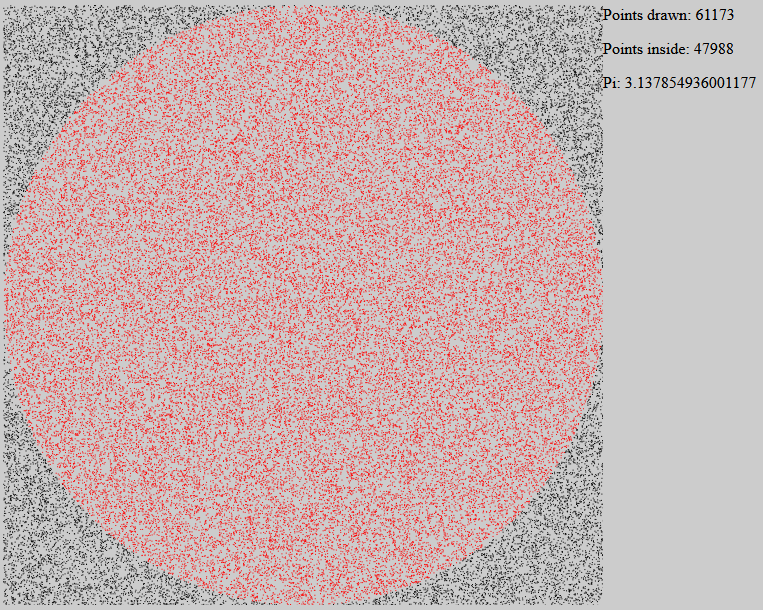
Take those two facts together and you can develop an experimental way to determine pi, called a Monte Carlo
method. Take a circle of radius 1 inside a square that exactly contains it. Then randomly choose points within the square. Statistically speaking, these random points have a
π/4 chance of occurring within the circle (rather than outside it). So if we take the number of points that lie within the circle, divide that by the total number of
points, and then multiply by 4, we should get something that approaches the value of pi. You could even do it by hand!
I wrote some software to do exactly that. Here’s what it looks like – the red points are inside the circle, and the black points are outside.
The software illustration I’ve written is raw JavaScript, HTML, and SVG, and should work in any modern web browser (though it can get a little slow once it’s drawn a few thousand
points!). Give it a go, here! When you go to that page, your browser will start drawing dots at random points, colouring them red if
the sum of the squares of their coordinates is less than 1, which is the radius of the circle (and the width of the square that encompasses it). As it goes along, it uses the formula I
described above to approximate the value of pi. You’ll probably get as far as 3.14 before you get bored, but there’s no reason that this method couldn’t be used to go as far as
you like: it’s not the best tool for the job, but it’s super-easy to understand and explain.
Oh, and it’s all completely open-source, so you’re welcome to take it and do with it what you wish. Turn off the graphical output
to make it run faster, and see if you can get an accurate approximation to 5 digits of pi! Or slow it down so you can see how the appearance of each and every point affects the
calculation. Or adapt it into a teaching tool and show your maths students one way that pi can be derived experimentally. It’s all yours: have fun.
And I’ll update you on my health at some other point.
So yeah: that’s not entirely pleasant. A couple of days ago I was diagnosed with what was supposed to be a minor bladder infection and given antibiotics. Then yesterday I became
feverish and collapsed. And now I’m in hospital.
But on the upside, they’ve spent all night pumping me full of some kind of intravaenous antibiotic that must be made from like unicorn spunk and leprechaun tears or something
because it’s frankly magical: feeling so much better today than yesterday.
I’m pretty sure that an outside observer, given the advance knowledge of this blog post, could easily tell when I’m in the process of getting over an illness just by the food I eat. I’m
pretty sure that I have a particular ‘tell’ in the foods I look for when I’m on the cusp of recovering from a cold, like now: or, I suppose, on those rare occasions that I’ll have drunk
enough to be suffering from a hangover.
Take this lunchtime, for example. I’ve been off work for the last couple of days, laid low by what seems to be the very same cold that I was sure I’d dodged when everybody else got it,
last month (I blame Annabel, the contagious little beast, who’s particularly keen on shoving her hands into people’s mouths). Today I’m back on my feet, but working from home: I skipped
breakfast, but by lunchtime I felt able to face some food, and quickly determined what it was that I really wanted:
An egg and cheese wafflestack. If you think it looks calorie-laden and disgusting, then you’re right: but you wouldn’t be saying that if you were recovering from an illness!
Egg & Cheese Wafflestack
Serves: 1 unwell-but-recovering person
Preparation: 15 minutes
Difficulty: if you can’t make this, get the hell out of the kitchen
Ingredients
4 × frozen potato waffles. I’m using Birds Eye ones, but honestly, who can tell the difference?
~ 30g mature cheddar cheese, grated or thinly sliced, brought to room temperature so it melts quickly
2 × eggs
A little vegetable oil
Tomato ketchup (alternatively, brown sauce works well)
Method
Grill the waffles in accordance with the instructions. Meanwhile, fry the two eggs (“sunny side up”: keep the yolk fluid). Assemble in stacks, with each stack consisting of cheese
sandwiched between two waffles, topped with an egg and the ketchup. Serve immediately. Eat as quickly as you dare.
So now I’m sitting here eating the taste of delicious recovery, generating 4096-bit strong probable prime numbers (like you do), and reading the feedback on a browser plugin I released recently. And every part of that is a huge
improvement upon lying ill in bed.
The seventh of my reviews of Godzilla Huntley’s (CaptainAvAngel) weekly Family Vlog, “IRL”, which features a not-very-well-hidden link to a secret bonus review video. Keep an eye out for it!






















{kind=link}