Chlorine
Low road or high road?
World War I. Gas in trenches.
Or salt shared, tears shed.
A haiku for every element on the periodic table up to atomic weight 103, and also one for the as-yet-unsynthesised ununennium, I especially like magnesium’s.
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
Chlorine
Low road or high road?
World War I. Gas in trenches.
Or salt shared, tears shed.
A haiku for every element on the periodic table up to atomic weight 103, and also one for the as-yet-unsynthesised ununennium, I especially like magnesium’s.
An increasing number of people are reportedly suffering from an allergy to the meat and other products of nonhuman mammals, reports Mosaic Science this week, and we’re increasingly confident that the cause is a sensitivity to alpha-gal (Galactose-alpha-1,3-galactose), a carbohydrate produced in the bodies of virtually all mammals except for us and our cousin apes, monkeys, and simians (and one of the reasons you can’t transplant tissue from pigs to humans, for example).

The interesting thing is that the most-common cause of alpha-gal sensitivity appears to be the bite of one of a small number of species of tick. The most-likely hypothesis seems to be that being bitten by such a tick after it’s bitten e.g. deer or cattle may introduce that species’ alpha-gal directly to your bloodstream. This exposure triggers an immune response through all future exposure, even if it’s is more minor, e.g. consuming milk products or even skin contact with an animal.
That’s nuts, isn’t it? The Mosaic Science article describes the reaction of Tami McGraw, whose symptoms began in 2010:
[She] asked her doctor to order a little-known blood test that would show if her immune system was reacting to a component of mammal meat. The test result was so strongly positive, her doctor called her at home to tell her to step away from the stove.
That should have been the end of her problems. Instead it launched her on an odyssey of discovering just how much mammal material is present in everyday life. One time, she took capsules of liquid painkiller and woke up in the middle of the night, itching and covered in hives provoked by the drug’s gelatine covering.
When she bought an unfamiliar lip balm, the lanolin in it made her mouth peel and blister. She planned to spend an afternoon gardening, spreading fertiliser and planting flowers, but passed out on the grass and had to be revived with an EpiPen. She had reacted to manure and bone meal that were enrichments in bagged compost she had bought.

Of course, this isn’t the only nor even the most-unusual (or most-severe) animal-induced allergy-to-a-different-animal we’re aware of. The hilariously-named but terribly-dangerous Pork-Cat syndrome is caused, though we’re not sure how, by exposure to cats and results in a severe allergy to pork. But what makes alpha-gal sensitivity really interesting is that it’s increasing in frequency at quite a dramatic rate. The culprit? Climate change. Probably.
It’s impossible to talk to physicians encountering alpha-gal cases without hearing that something has changed to make the tick that transmits it more common – even though they don’t know what that something might be.
…
“Climate change is likely playing a role in the northward expansion,” Ostfeld adds, but acknowledges that we don’t know what else could also be contributing.
To take a minor diversion: another article I saw this week was the BBC‘s one on the climate footprint of the food you eat.
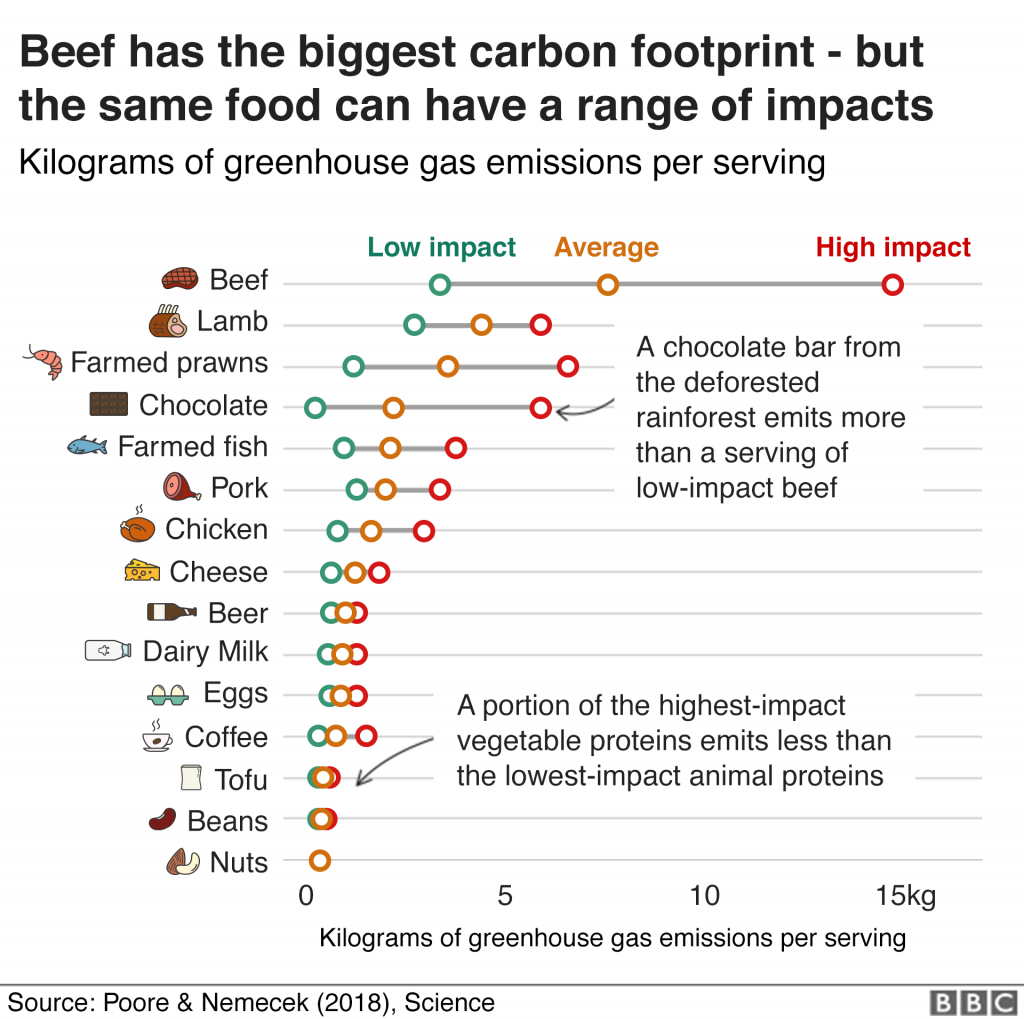
A little dated, perhaps: I’m sure that nobody needs to be told nowadays that one of the biggest things a Westerner can do to reduce their personal carbon footprint (after from breeding less or not at all, which I maintain is the biggest, or avoiding air travel, which Statto argues for) is to reduce or refrain from consumption of meat (especially pork and beef) and dairy products.
Indeed, environmental impact was the biggest factor in my vegetarianism (now weekday-vegetarianism) for the last eight years, and it’s an outlook that I’ve seen continue to grow in others over the same period.
Seeing these two stories side-by-side in my RSS reader put the Gaia hypothesis in my mind.
If you’re not familiar with the Gaia hypothesis, the basic idea is this: by some mechanism, the Earth and all of the life on it act in synergy to maintain homeostasis. Organisms not only co-evolve with one another but also with the planet itself, affecting their environment in a way that in turn affects their future evolution in a perpetual symbiotic relationship of life and its habitat.
Its advocates point to negative feedback loops in nature such as plankton blooms affecting the weather in ways that inhibit plankton blooms and to simplistic theoretical models like the Daisyworld Simulation (cute video). A minority of its proponents go a step further and describe the Earth’s changes teleologically, implying a conscious Earth with an intention to protect its ecosystems (yes, these hypotheses were born out of the late 1960s, why do you ask?). Regardless, the essence is the same: life’s effect on its environment affects the environment’s hospitality to life, and vice-versa.
There’s an attractive symmetry to it, isn’t there, in light of the growth in alpha-gal allergies? Like:

That’s not to say that I buy it, mind. The Gaia hypothesis has a number of problems, and – almost as bad – it encourages a complacent “it’ll all be okay, the Earth will fix itself” mindset to climate change (which, even if it’s true, doesn’t bode well for the humans residing on it).
But it was a fun parallel to land in my news reader this morning, so I thought I’d share it with you. And, by proxy, make you just a little bit warier of ticks than you might have been already. /shudders/
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
Quantum computing is all the rage. It seems like hardly a day goes by without some news outlet describing the extraordinary things this technology promises. Most commentators forget, or just gloss over, the fact that people have been working on quantum computing for decades—and without any practical results to show for it.
We’ve been told that quantum computers could “provide breakthroughs in many disciplines, including materials and drug discovery, the optimization of complex manmade systems, and artificial intelligence.” We’ve been assured that quantum computers will “forever alter our economic, industrial, academic, and societal landscape.” We’ve even been told that “the encryption that protects the world’s most sensitive data may soon be broken” by quantum computers. It has gotten to the point where many researchers in various fields of physics feel obliged to justify whatever work they are doing by claiming that it has some relevance to quantum computing.
Meanwhile, government research agencies, academic departments (many of them funded by government agencies), and corporate laboratories are spending billions of dollars a year developing quantum computers. On Wall Street, Morgan Stanley and other financial giants expect quantum computing to mature soon and are keen to figure out how this technology can help them.
It’s become something of a self-perpetuating arms race, with many organizations seemingly staying in the race if only to avoid being left behind. Some of the world’s top technical talent, at places like Google, IBM, and Microsoft, are working hard, and with lavish resources in state-of-the-art laboratories, to realize their vision of a quantum-computing future.
In light of all this, it’s natural to wonder: When will useful quantum computers be constructed? The most optimistic experts estimate it will take 5 to 10 years. More cautious ones predict 20 to 30 years. (Similar predictions have been voiced, by the way, for the last 20 years.) I belong to a tiny minority that answers, “Not in the foreseeable future.” Having spent decades conducting research in quantum and condensed-matter physics, I’ve developed my very pessimistic view. It’s based on an understanding of the gargantuan technical challenges that would have to be overcome to ever make quantum computing work.
…
Great article undermining all the most-widespread popular arguments about how quantum computing will revolutionise aboslutely everything, any day now. Let’s stay realistic, here: despite all the hype, it might well be the case that it’s impossible to build a quantum computer of sufficient complexity to have any meaningful impact on the world beyond the most highly-experimental and theoretical applications. And even if it is possible, its applications might well be limited: the “great potential” they carry is highly hypothetical.
Don’t get me wrong, I’m super excited about the possibility of quantum computing, too. But as Mickhail points out, we must temper our excitement with a little realism and not give in to the hype.
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
Why are testicles kept in a vulnerable dangling sac? It’s not why you think.
…
Some of you may be thinking that there is a simple answer: temperature. This arrangement evolved to keep them cool. I thought so, too, and assumed that a quick glimpse at the scientific literature would reveal the biological reasons and I’d move on. But what I found was that the small band of scientists who have dedicated their professional time to pondering the scrotum’s existence are starkly divided over this so-called cooling hypothesis.
…
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
Fabulous explanation of the Strong Equivalence Principle coupled with a nice bit of recent research to prove that it holds true even in extreme gravitational fields (and therefore disproving a few interesting fringe theories). It’s hard science made to enjoy like pop science: yay! Plus a Hitch-Hiker’s Guide to the Galaxy reference, to boot. Under 10,000 views; go show them some love.
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
I’m not sure that there’s any age that’s too-young at which to try to cultivate an interest in science. Once a child’s old enough to ask why something is the case, every question poses an opportunity for an experiment! Sometimes a thought experiment is sufficient (“Uncle Dan: why do dogs not wear clothes?”) but other times provide the opportunity for some genuine hands-on experimentation (“Why do we put flowers in water?”). All you have to do is take every question and work out what you’d do if you didn’t know the answer either! A willingness to take any problem with a “let’s find out” mentality teaches children two important things: (a) that while grown-ups will generally know more than them, that nobody has all the answers, and (b) that you can use experiments to help find the answers to questions – even ones that have never been asked before!

Sometimes it takes a little more effort. Kids – like all of us, a lot of the time – can often be quite happy to simply accept the world as-it-is and not ask “why”. But because a fun and educational science activity is a good way to occupy a little one (and remember: all it needs to be science is to ask a question and then try to use evidence to answer it!), I’ve been keeping a list of possible future activities so that we’ve got a nice rainy-day list of things to try. And because we are, these days, in an increasingly-large circle of breeders, I thought I’d share some with you.

Here’s some of the activities we’ve been doing so far (or that I’ve got lined-up for future activities as and when they become appropriate):






So there’s my “now and next” list of science activities that we’ll be playing at over the coming months. I’m always open to more suggestions, though, so if you’re similarly trying to help shape an enquiring and analytical mind, let me know what you’ve been up to!
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
This is a repost promoting content originally published elsewhere. See more things Dan's reposted.
On August 27, 1883, the Earth let out a noise louder than any it has made since…
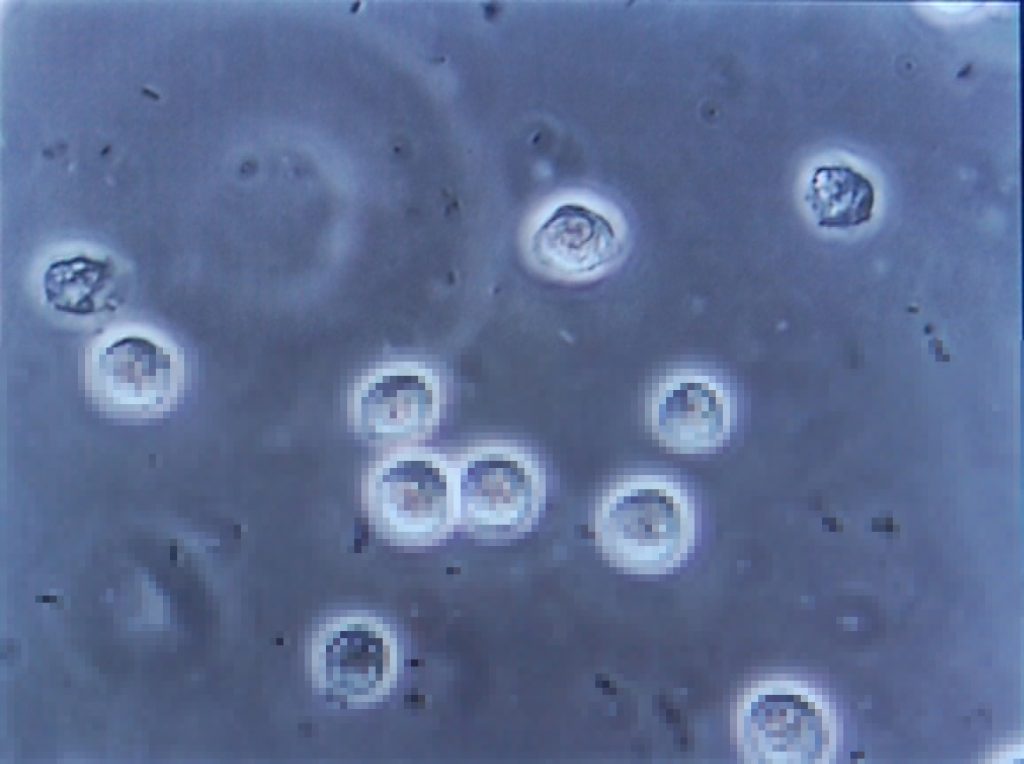
Warning: this blog post contains pictures of urine, invasive equipment, and the inside of a bladder. It’s probably safe for all audiences, but you might like to put your glass of apple juice down for a minute or two. The short of it all is that I’m probably healthy.
Since my hospitalisation the other month with a renal system infection, I’ve undergone a series of investigations to try to determine if there’s an underlying reason that I fell ill. As my doctor explained to me, it’s quite possible that what I’d experienced was a random opportunistic infection (perhaps aided by a course of unrelated antibiotics I’d been on earlier this year or by certain lifestyle habits), but if that wasn’t the case – if there were some deeper explanation for my health problems – it was important to find out sooner, rather than later.
Early on I had several ultrasound scans of my bladder (at a number of different times and at a variety of levels of fullness) and one of my kidneys, the latter of which revealed some “minor scarring” of one of them which apparently isn’t something I should be worried about… although I wish they’d started the two-page letter I got with that rather than opening with, effectively, “Contrary to what we told you at the hospital, we did later see something wrong with you…” But still, good to be reassured that this is probably not an issue.

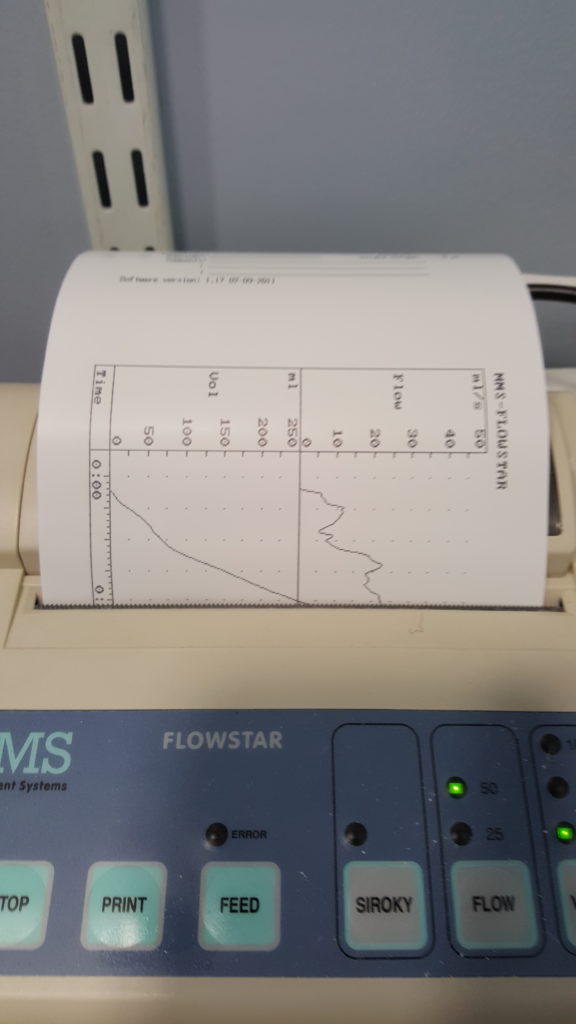
More recently, I went to the hospital to have a “flow rate test” and a cystoscopy. The flow rate test involved the most-ghetto looking piece of NHS equipment I’ve ever seen: functionally, it seemed to be little more than a funnel on top of a large measuring beaker, in turn on top of a pressure-sensitive digital scale. The scale was connected up to the only fancy-looking bit of equipment in the room, a graphing printer that output the calculated volume (based on their weight) of the same and, more-importantly, the rate of change: the “flow rate” of the stream of urine.

I suppose one advantage of using equipment like this is that it basically operates itself. Which meant that the nurse was able to give me five seconds worth of instruction and then leave the room, which saved us from our own Britishness forcing us to make small-talk while I urinated in front of her or something. Ultimately, I turned out to be within the range of normalcy here, too, although I was a little disappointed to find that the ward didn’t maintain a daily “score board” of flow rates, as sort-of a science-backed literal pissing contest.
Finally came the cystoscopy, and this was the bit that I’d been most-nervous about. This procedure involves the insertion of a long flexible tube into the urethra at the tip of the penis, under local anasthetic, and pushing it all the way down, through the sphincter, down through the prostate and then back up into the bladder. It’s then used as a channel to pump water into the bladder, filling it to capacity and stretching out the sides, after which the fibreoptic cord (and light) that runs along its length is used to look around inside the bladder to inspect for any of a plethora of different problems.

The doctor invited me to watch with him on the monitor, which I initially assumed was because I was clearly interested in everything and kept asking questions, but in hindsight I wonder if it’s just that he – quite rightly – assumed that I might have panicked if I’d have been looking in the direction of the piece of equipment he brought in and jabbed at my penis with. I only looked at it while it was on its way out, and my god its a scary-looking thing: sort of like a cross between a tyre pressure gauge and a blowtorch. The first few inches were painless – the local anasthetic had made me completely numb right up to and including the external sphincter, which is at the base of the penis. However, what I can only assume was the second sphincter complained of the discomfort, and it stung pretty sharply any time the doctor would twist the cystoscope to change the angle of the picture.
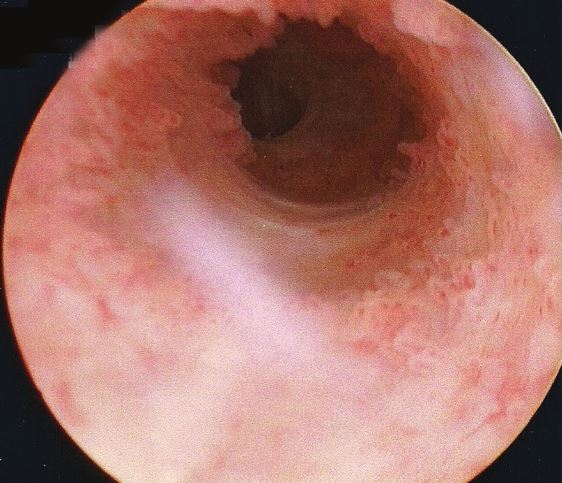
Seeing the inside of your own body is an amazing experience. I mean: it’s not amazing enough to even be worth the experience of a cystoscopy, never mind the illness that in my case preceeded it… but it’s still pretty cool. The ultrasounds were interesting, but there’s nothing quite so immersive as seeing a picture of the inside of your own bladder, gritting your teeth while the doctor points to an indentation and explains that it’s the opening to the ureter that connects to your own left kidney!
Unfortunately I neglected to take my phone into the operating room, having put it into a locker when I changed into a gown, and so I wasn’t able to (as I’d hoped) take photos of the inside of my own bladder. So you’ll have to make do with this video I found, which approximates the experience pretty well. The good news is that there’s probably nothing wrong with me, now that the infection from earlier this year has passed: nothing to suggest that there’s any deeper underlying issue that caused me to get sick, anyway!
The bad news is that while the procedure itself was shorter and more-bearable than I’d expected, the recovery’s been a real drag. A week later, it still hurts a lot to urinate (although I’ve stopped yelping out loud when I do so) and my crotch is still too sore for me to be able to cycle. I’ve also discovered that an errection can be painful enough to wake me up, which is definitely not the most-pleasant way I’ve been roused by a penis. But it’s getting better, day by day, and at least I know for sure that I’m more-or-less “right” in the renal system, now.
As I mentioned last week, I’ve been ill. For those who wanted the grisly details, well: here you go.
Warning: this blog post contains frank subjective descriptions of the symptoms of slightly-icky medical conditions including photographs. It’s probably safe for all audiences, but you might not want to be drinking anything while you read it.
The trouble began, I suppose, about a month and a half ago, when a contracted what seemed to be a minor urinary tract infection. If you’re a woman then, statistically-speaking, I probably don’t need to tell you what that is, but for the benefit of the men: it’s what happens when bacteria (or, sometimes, a fungus or virus) infects the renal system: the kidneys, bladder, ureters, and especially the urethra. It’s not pleasant: it gives you the feeling of needing to pee the whole time, makes it harder to pee, and – when you do – it feels a little bit like you’re piss is made of lava.
Despite it not being common for men (more on that later), I’ve had mild UTIs on a couple of occasions in my life, and I’d always found that ensuring that I got plenty of water and a full RDA of vitamin C was more than enough to make it clear up all by itself within a couple of days. So that’s what I started doing. But then things took a turn for the worse: I started getting a stabbing pain in my left kidney. Recognising this as being pyelonephritis, I went to the doctor who prescribed me a course of the antibiotic ciprofloxacin. Within a couple of days I was feeling right as rain (of course I continued to finish the course of drugs, although I was interested to see that that advice is starting to become controversial).

Naturally I was a little disappointed when, the week before last, I started getting UTI-like pain again, followed very swiftly this time by pain in my bladder that constantly felt a little like I was recovering from being punched. Back to the doctor I went, where (after the usual tests to work out what the most-likely best-antibiotic to use was) I was prescribed a course of nitrofurantoin. I’d never had this particular drug before, and it wasn’t initially clear which of the escalating ill-effects I was experiencing were symptoms of the infection and which were side-effects of the medication: it started with joint pain, then nausea, then diarrhoea, then a full-on fever. It was at the point that I was fully-clothed in bed, running a temperature and soaked in sweat but still feeling cold and shivering that Ruth called 111, who told her to take me to A&E.
(Which, like her care for me in general, she did fabulously well, except for a little bit where she sort-of ran me over in the car park of the hospital: thankfully some friendly paramedics were standing around and were able to drag me into the building. Anyway, I don’t have much memory of that bit and I certainly don’t have any amusing photos, so I’ll skip over it.)

A few tests later, the medical staff seemed confident that what I was experiencing was not an allergic reaction to the antibiotic (however, I see that they still made a note of it as a risk on my notes!) but was a progression of the infection, which seemed to have crossed over from the tissues of my renal system and into my bloodstream and was now generally causing havoc by attacking the rest of my body. They hooked me up to a drip of an intravenous antibiotic and kept me stocked with painkillers, then sent me up to the urology ward and set me up with a “bed” (urology mostly deals with outpatients, and so my ‘bed’ was actually a trolley, but they wanted to keep me close to the urologists in case of any complications).

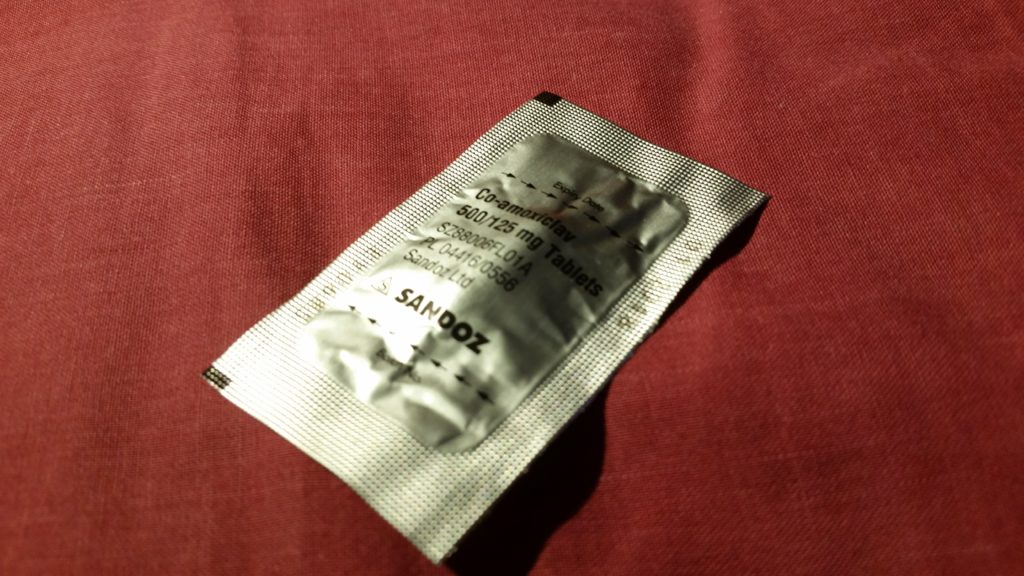
A consultant switched me to a week’s course of yet-another different antibiotic – co-amoxiclav – and recommended keeping me in for another night. Now, I think that co-amoxiclav is a really interesting drug, so I’m going to be a bit of a nerd and tell you about that for a bit (I promise we’ll get back to my health in a moment: if you don’t want the science bit, just scroll past the diagrams to the next photo).
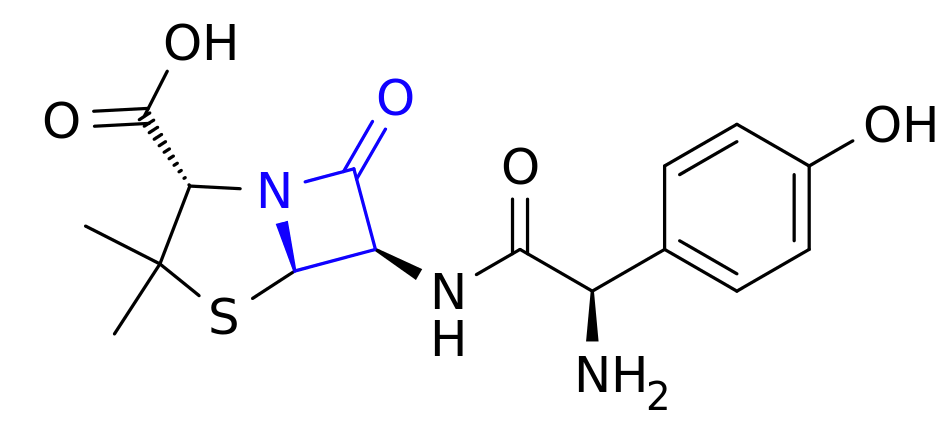
Co-amoxiclav is a mixture of two drugs. The first is the antibiotic amoxicillin. Amoxicillin belongs to a class of antibiotics (which includes penicillin) called β-lactams, which is the most-commonly used family of antibiotics. These antibiotics contain a four-point lactam ‘ring’ (highlighted in blue above), and the way that they work is that this part of the molecule bonds with a particular protein common to all gram-positive bacteria. Normally this protein is responsible for producing peptidoglycan, which is an essential ingredient in the cell walls of these kinds of bacteria, but when it gets locked to a β-lactam ring it stops working. As a result, when the bacterium reproduces the new child doesn’t have a proper cell wall, and can’t survive long in even the least-hostile environments.
Of course, we’re in a medical arms race right now because some of the bacteria which we’re targetting with antibiotics are becoming resistant. And here’s one what that they’re doing so: some of these bacteria have evolved to produce beta-lactamase, also bonds with beta-lactam rings, adding an OH to them and making them useless. Bummer, eh?
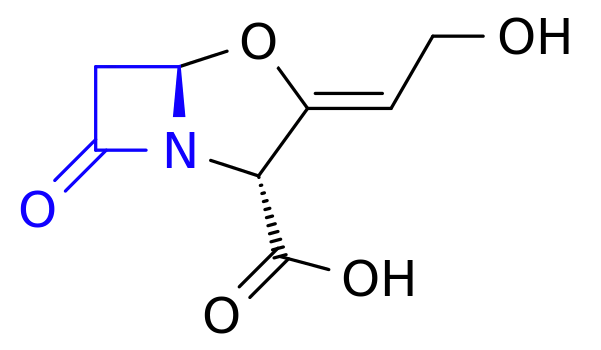
The second drug in co-amoxiclav, then, is clavulanic acid, which was discovered in the 1970s and started being added to drugs in the 1980s. Despite having a β-lactam ring (as you’ll see in blue above), clavulanic acid by itself it isn’t an effective antibiotic (for reasons I can’t quite get my head around – anyone want to help me?). But what it’s great at is bonding that lactam ring to beta-lactamase, thereby deactivating the bacterial counter-offensive and allowing the amoxicillin to carry on working, combating resistance.
So what you’ve got in co-amoxiclav is a an antibiotic and a chemical that counteracts the effects of a chemical that deactivates that antibiotic. Wow! It’s things like this that really make me wish I had a brain for biology!

I was eventually discharged from hospital and released to go home for lots of bed rest and water, along with a further week’s course of co-amoxiclav. Unfortunately it turns out that I’m one of the unlucky folks for whom amoxicillin makes me dizzy, so I spent most of that week lying down in-between wobbly vertigo-filled trips to and from the bathroom. But it worked! Within a few days I was feeling much better and by the end of last week I was able to work from home (and actually feel like I was useful again!).
Free of symptoms and off the drugs, I returned to work properly on Monday morning and everything seemed fine. Until, late in the morning, I went to the bathroom and started pissing blood.

Now apparently blood in your urine, while horrifying when it happens to you unexpectedly, isn’t actually a sign of a medical emergency. I was starting to get bladder pain again, quite intensely, so I excused myself from work and called the urology ward, who decided that I wasn’t in bad enough a condition to go and see them but sent me straight to my GP, who gave me another fortnight’s worth of co-amoxiclav. They’re monitoring my progress with urine and blood samples and if by Friday it’s not having an impact, they’re going to want to send me back to hospital (hopefully only as an outpatient) and pump me full of the intravenous stuff again. So… fingers crossed for a good result out of these drugs.
I was hoping that by this point I’d be writing this blog post and telling you all about how I’d fought the bladder monster and won. But it looks like I won’t be able to claim that victory for another week or two, yet. All I know is that I searched for “bladder monster” and found this. Yeah: that feels about right.
This self-post was originally posted to /r/askscience. See more things from Dan's Reddit account.
Wind and brass instruments (which I’ve just learned are collectively ‘aerophones’) work because since characteristic of their shape causes the air that is pushed or drawn through them to vibrate at particular frequencies. They work in air whether you’re down a mine or at the top of a mountain, so there’s clearly some tolerance to pressure variation. I presume, therefore, that you could play them using other gases too (e.g. by connecting a whistle to a pump in a nitrogen atmosphere, for example), albeit presumably with a change in pitch (we have whistles driven by an air/steam mixture on steam locomotives, for example).
But I wonder: can such an instrument be used with other fluids? How about a liquid, like water? Can I pump water through an underwater whistle in order to make a whistle-like noise? What are the physical constraints on doing so (e.g do I need a higher pressure difference in water)?
If it’s not possible, why not? What could be done, hypothetically, to construct an aerophone-style (“hydrophone”?) instrument that would work underwater?
tl;dr: Could I pump water through an underwater whistle to ‘blow’ it? If not, how can I ‘fix’ that?
This link was originally posted to /r/Experimentally. See more things from Dan's Reddit account.
The original link was: https://www.youtube.com/watch?v=GwzUMEuGZHs
This self-post was originally posted to /r/askscience. See more things from Dan's Reddit account.
I’ve just finished a long work week, got home, and made a gin and tonic, and I’m looking at the ice cubes bobbing in it and noticed something I’d not paid attention to before: the cubes seem to be opaque in their core but more-transparent towards their crust. You can see what I mean in this photo.
Now other photos, like this one, show that the effect isn’t universal (and I’m pretty sure I’ve seen perfectly clear ice cubes before, too). So… why are mine opaque?
If it helps:
Thanks!
This self-post was originally posted to /r/askscience. See more things from Dan's Reddit account.
I was elsewhere in Reddit when somebody made the claim that the space between the spiral arms of our galaxy aren’t empty, but are simply filled with different kinds of stars (different luminoscities, etc.). I was skeptical, but other sources claim that this is true, too. However, I can’t find any explanation as to why this might be the case.
Is our galaxy unusual in this regard? Is it that stars form throughout our galaxy, but matter ejected from the bar into the arms affects the type of stars seen there? Is this a question of what forms where, or is it a clustering question? I honestly haven’t a clue, and I couldn’t find where this question had been asked before so I’m still “in the dark”… unlike the ‘dark’ places in our galaxy!
{kind=link}
{kind=link}